

Copeptin and risk stratification in patients with acute dyspnea
- PMID: 21106053
- PMCID: PMC3220005
- DOI: 10.1186/cc9336
Copeptin and risk stratification in patients with acute dyspnea
Abstract
Introduction: The identification of patients at highest risk for adverse outcome who are presenting with acute dyspnea to the emergency department remains a challenge. This study investigates the prognostic value of Copeptin, the C-terminal part of the vasopressin prohormone alone and combined to N-terminal pro B-type natriuretic peptide (NT-proBNP) in patients with acute dyspnea.
Methods: We conducted a prospective, observational cohort study in the emergency department of a university hospital and enrolled 287 patients with acute dyspnea.
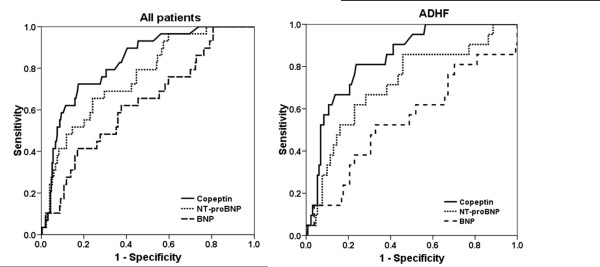
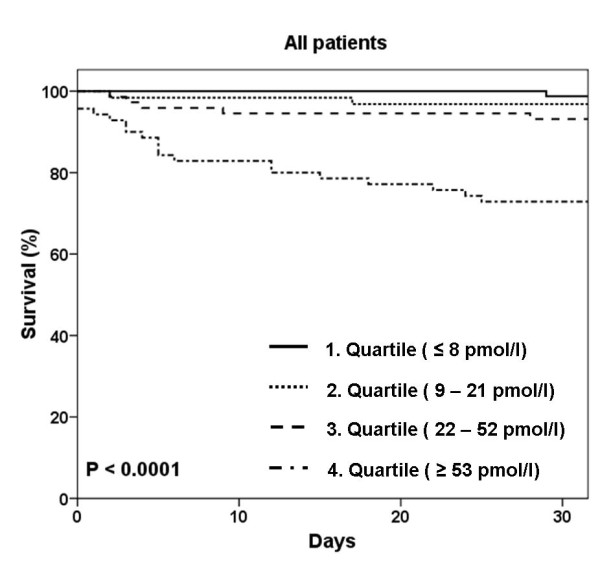
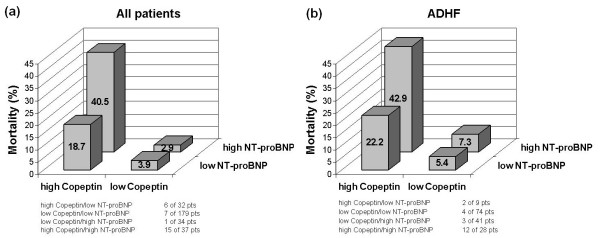
Results: Copeptin levels were elevated in non-survivors (n = 29) compared to survivors at 30 days (108 pmol/l, interquartile range (IQR) 37 to 197 pmol/l) vs. 18 pmol/l, IQR 7 to 43 pmol/l; P < 0.0001). The areas under the receiver operating characteristic curve (AUC) to predict 30-day mortality were 0.83 (95% confidence interval (CI) 0.76 to 0.90), 0.76 (95% CI 0.67 to 0.84) and 0.63 (95% CI 0.53 to 0.74) for Copeptin, NT-proBNP and BNP, respectively (Copeptin vs. NTproBNP P = 0.21; Copeptin vs. BNP P = 0.002). When adjusted for common cardiovascular risk factors and NT-proBNP, Copeptin was the strongest independent predictor for short-term mortality in all patients (HR 3.88 (1.94 to 7.77); P < 0.001) and especially in patients with acute decompensated heart failure (ADHF) (HR 5.99 (2.55 to 14.07); P < 0.0001). With the inclusion of Copeptin to the adjusted model including NTproBNP, the net reclassification improvement (NRI) was 0.37 (P < 0.001). An additional 30% of those who experienced events were reclassified as high risk, and an additional 26% without events were reclassified as low risk.
Conclusions: Copeptin is a new promising prognostic marker for short-term mortality independently and additive to natriuretic peptide levels in patients with acute dyspnea.
Figures

Similar articles
-
Midregional pro-adrenomedullin in addition to b-type natriuretic peptides in the risk stratification of patients with acute dyspnea: an observational study.Crit Care. 2009;13(4):R122. doi: 10.1186/cc7975. Epub 2009 Jul 23. Crit Care. 2009. PMID: 19627611 Free PMC article.
-
C-terminal provasopressin (copeptin) as a novel and prognostic marker in acute myocardial infarction: Leicester Acute Myocardial Infarction Peptide (LAMP) study.Circulation. 2007 Apr 24;115(16):2103-10. doi: 10.1161/CIRCULATIONAHA.106.685503. Epub 2007 Apr 9. Circulation. 2007. PMID: 17420344 Clinical Trial.
-
Lack of diagnostic and prognostic utility of circulating plasma myeloperoxidase concentrations in patients presenting with dyspnea.Clin Chem. 2009 Jan;55(1):59-67. doi: 10.1373/clinchem.2008.108159. Epub 2008 Nov 6. Clin Chem. 2009. PMID: 18988754
-
Amino-terminal pro-B-type natriuretic peptide testing and prognosis in patients with acute dyspnea, including those with acute heart failure.Am J Cardiol. 2008 Feb 4;101(3A):49-55. doi: 10.1016/j.amjcard.2007.11.020. Am J Cardiol. 2008. PMID: 18243859 Review.
-
Copeptin in heart failure: Review and meta-analysis.Clin Chim Acta. 2017 Dec;475:36-43. doi: 10.1016/j.cca.2017.10.001. Epub 2017 Oct 2. Clin Chim Acta. 2017. PMID: 28982590 Review.
Cited by
-
Plasma concentrations of the vasoactive peptide fragments mid-regional pro-adrenomedullin, C-terminal pro-endothelin 1 and copeptin in hemodialysis patients: associated factors and prediction of mortality.PLoS One. 2014 Jan 22;9(1):e86148. doi: 10.1371/journal.pone.0086148. eCollection 2014. PLoS One. 2014. PMID: 24465926 Free PMC article.
-
Predictive value of plasma copeptin level for the risk and mortality of heart failure: a meta-analysis.J Cell Mol Med. 2017 Sep;21(9):1815-1825. doi: 10.1111/jcmm.13102. Epub 2017 Feb 28. J Cell Mol Med. 2017. PMID: 28244638 Free PMC article.
-
Prognostic role of copeptin with all-cause mortality after heart failure: a systematic review and meta-analysis.Ther Clin Risk Manag. 2017 Jan 5;13:49-58. doi: 10.2147/TCRM.S124689. eCollection 2017. Ther Clin Risk Manag. 2017. PMID: 28115852 Free PMC article.
-
Copeptin as a New Blood-Based Marker for Differential Diagnosis in Stroke Patients.Int J Mol Sci. 2025 Jun 1;26(11):5328. doi: 10.3390/ijms26115328. Int J Mol Sci. 2025. PMID: 40508137 Free PMC article. Review.
-
Cortisol as a prognostic marker of short-term outcome in chinese patients with acute ischemic stroke.PLoS One. 2013 Sep 12;8(9):e72758. doi: 10.1371/journal.pone.0072758. eCollection 2013. PLoS One. 2013. Retraction in: PLoS One. 2022 Mar 30;17(3):e0266461. doi: 10.1371/journal.pone.0266461. PMID: 24069157 Free PMC article. Retracted.
References
-
- Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, Omland T, Storrow AB, Abraham WT, Wu AH, Clopton P, Steg PG, Westheim A, Knudsen CW, Perez A, Kazanegra R, Herrmann HC, McCullough PA. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161–167. doi: 10.1056/NEJMoa020233. - DOI - PubMed
-
- Dyspnea. Mechanisms, assessment, and management: a consensus statement. American Thoracic Society. Am J Respir Crit Care Med. 1999;159:321–340. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
