

Ambivalent connections: a qualitative study of the care experiences of non-psychotic chronic patients who are perceived as 'difficult' by professionals
- PMID: 21106084
- PMCID: PMC3002895
- DOI: 10.1186/1471-244X-10-96
Ambivalent connections: a qualitative study of the care experiences of non-psychotic chronic patients who are perceived as 'difficult' by professionals
Abstract
Background: Little is known about the perspectives of psychiatric patients who are perceived as 'difficult' by clinicians. The aim of this paper is to improve understanding of the connections between patients and professionals from patients' point of view.
Methods: A Grounded Theory study using interviews with 21 patients from 12 outpatient departments of three mental health care facilities.
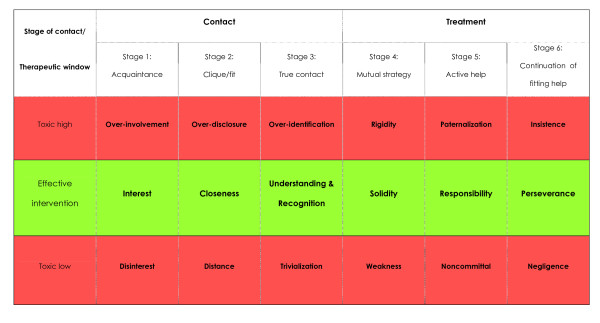
Results: Patients reported on their own difficult behaviours and their difficulties with clinicians and services. Explanations varied but could be summarized as a perceived lack of recognition. Recognition referred to being seen as a patient and a person - not just as completely 'ill' or as completely 'healthy'. Also, we found that patients and professionals have very different expectations of one another, which may culminate in a difficult or ambivalent connection. In order to explicate patient's expectations, the patient-clinician contact was described by a stage model that differentiates between three stages of contact development, and three stages of substantial treatment. According to patients, in each stage there is a therapeutic window of optimal clinician behaviour and two wider spaces below and above that may be qualified as 'toxic' behaviour. Possible changes in clinicians' responses to 'difficult' patients were described using this model.
Conclusions: The incongruence of patients' and professionals' expectations may result in power struggles that may make professionals perceive patients as 'difficult'. Explication of mutual expectations may be useful in such cases. The presented model gives some directions to clinicians how to do this.
Figures
Similar articles
-
How do patients come to be seen as 'difficult'?: a mixed-methods study in community mental health care.Soc Sci Med. 2011 Feb;72(4):504-12. doi: 10.1016/j.socscimed.2010.11.036. Epub 2010 Dec 16. Soc Sci Med. 2011. PMID: 21208704
-
Promoting and supporting self-management for adults living in the community with physical chronic illness: A systematic review of the effectiveness and meaningfulness of the patient-practitioner encounter.JBI Libr Syst Rev. 2009;7(13):492-582. doi: 10.11124/01938924-200907130-00001. JBI Libr Syst Rev. 2009. PMID: 27819974
-
Problems in psychiatric care of 'difficult patients': a Delphi-study.Epidemiol Psichiatr Soc. 2009 Oct-Dec;18(4):323-30. Epidemiol Psichiatr Soc. 2009. PMID: 20170047
-
"Difficult patients" in mental health care: a review.Psychiatr Serv. 2006 Jun;57(6):795-802. doi: 10.1176/ps.2006.57.6.795. Psychiatr Serv. 2006. PMID: 16754755 Review.
-
Non-helpful relationships with professionals - a literature review of the perspective of persons with severe mental illness.J Ment Health. 2016 Jun;25(3):267-77. doi: 10.3109/09638237.2015.1101427. Epub 2015 Dec 14. J Ment Health. 2016. PMID: 27150468 Review.
Cited by
-
Decision making on (dis)continuation of long-term treatment in mental health services is an interpersonal negotiation rather than an objective process: qualitative study.BMC Psychiatry. 2019 Mar 18;19(1):92. doi: 10.1186/s12888-019-2072-0. BMC Psychiatry. 2019. PMID: 30885155 Free PMC article.
-
A patient perspective on recurrent or prolonged contact with psychiatric inpatient care for affective disorder.Int J Ment Health Syst. 2018 Jun 5;12:29. doi: 10.1186/s13033-018-0205-3. eCollection 2018. Int J Ment Health Syst. 2018. PMID: 29928292 Free PMC article.
-
Development of an intervention program to increase effective behaviours by patients and clinicians in psychiatric services: Intervention Mapping study.BMC Health Serv Res. 2010 Oct 25;10:293. doi: 10.1186/1472-6963-10-293. BMC Health Serv Res. 2010. PMID: 20973985 Free PMC article.
-
Snakes and Ladders: The experience of being referred to and seen by Child and Adolescent Mental Health Services.SSM Ment Health. 2024 Dec;6:100343. doi: 10.1016/j.ssmmh.2024.100343. SSM Ment Health. 2024. PMID: 39678451 Free PMC article.
References
-
- Lin EH, Katon W, Korff Von, Bush P, Lipscomb P, Russo J. et al.Frustrating patients: physician and patient perspectives among distressed high users of medical services. J Gen Intern Med. 1991;6:24124–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
