

The contemporary role of blood products and components used in trauma resuscitation
- PMID: 21106098
- PMCID: PMC3004811
- DOI: 10.1186/1757-7241-18-63
The contemporary role of blood products and components used in trauma resuscitation
Abstract
Introduction: There is renewed interest in blood product use for resuscitation stimulated by recent military experience and growing recognition of the limitations of large-volume crystalloid resuscitation.
Methods: An editorial review of recent reports published by investigators from the United States and Europe is presented. There is little prospective data in this area.
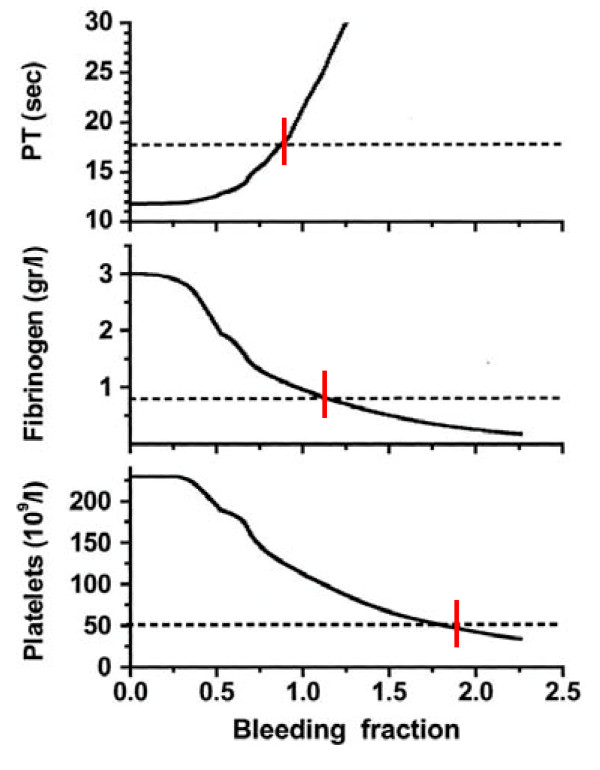
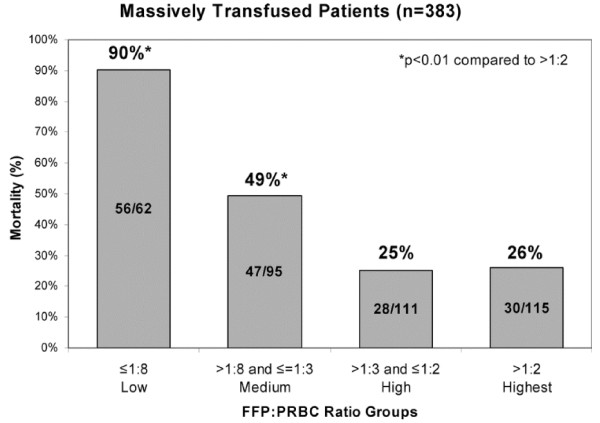
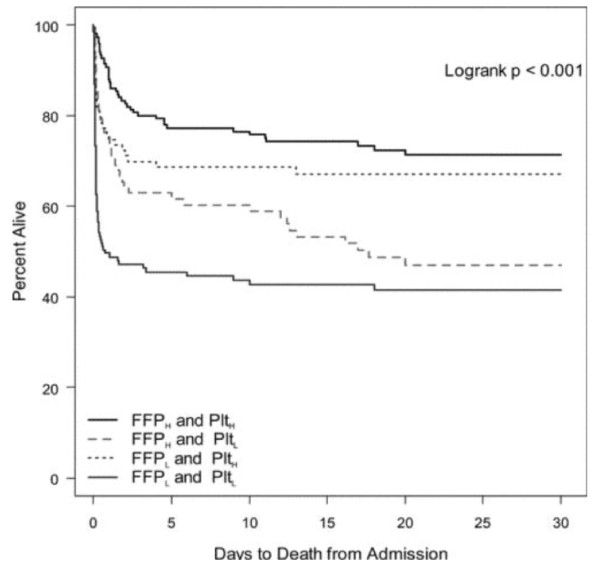
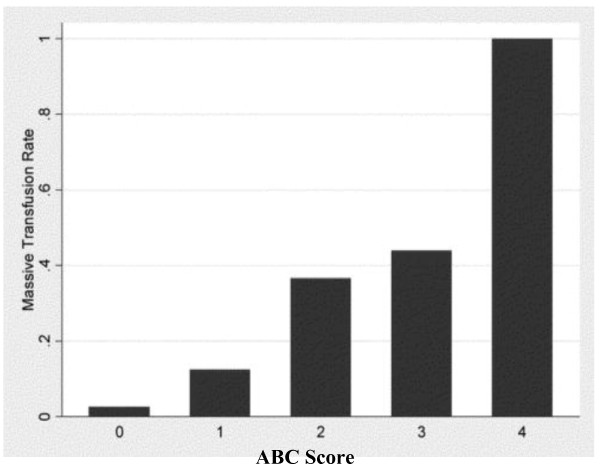
Results: Despite increasing sophistication of trauma care systems, hemorrhage remains the major cause of early death after injury. In patients receiving massive transfusion, defined as 10 or more units of packed red blood cells in the first 24 hours after injury, administration of plasma and platelets in a ratio equivalent to packed red blood cells is becoming more common. There is a clear possibility of time dependent enrollment bias. The early use of multiple types of blood products is stimulated by the recognition of coagulopathy after reinjury which may occur as many as 25% of patients. These patients typically have large-volume tissue injury and are acidotic. Despite early enthusiasm, the value of administration of recombinant factor VIIa is now in question. Another dilemma is monitoring of appropriate component administration to control coagulopathy.
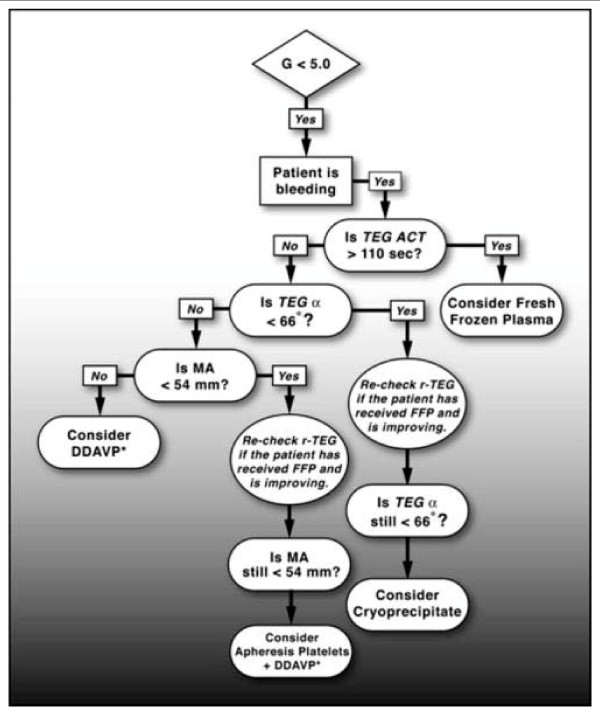
Conclusion: In patients requiring large volumes of blood products or displaying coagulopathy after injury, it appears that early and aggressive administration of blood component therapy may actually reduce the aggregate amount of blood required. If recombinant factor VIIa is given, it should be utilized in the fully resuscitated patient. Thrombelastography is seeing increased application for real-time assessment of coagulation changes after injury and directed replacement of components of the clotting mechanism.
Figures


References
-
- Simmons RL, Collins JA, Heisterkamp CA, Mills DE, Andren R, Phillips LL. Coagulation disorders in combat casualties. I. Acute changes after wounding. II. Effects of massive transfusion. III Post-resuscitative changes. Ann Surg. 1969;169:455–482. doi: 10.1097/00000658-196904000-00001. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
