

Private and public health care in rural areas of Uganda
- PMID: 21106099
- PMCID: PMC3003635
- DOI: 10.1186/1472-698X-10-29
Private and public health care in rural areas of Uganda
Abstract
Background: In many low and middle income countries, the private sector is increasingly becoming an important source of health care, filling gaps where no or little public health care is available. However, knowledge on the private sector providers is limited The objective of this study was to determine the type and number of different types of health care providers, and the quality, cost and utilization of care delivered by those providers in rural Uganda.
Methods: The study was carried out in three rural districts. Methods included (1) mapping of health care providers; (2) a household survey to determine morbidity and health care utilization; (3) a health facility survey to assess quality of care; (4) focus group discussions to get qualitative information on providers and provider choice; and (5) key informant interviews to further explore service characteristics.
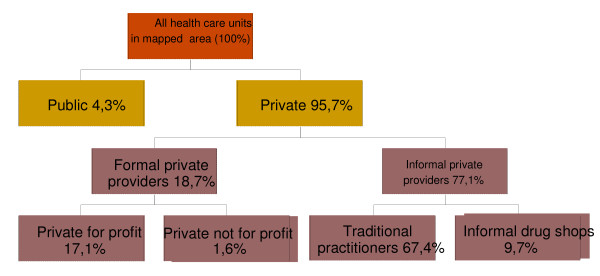
Results: 95.7% of all 445 facilities surveyed were private while 4.3% were public. Traditional practitioners and general merchandise shops that sold medicines comprised 77.1% of all providers. They had limited infrastructure and skills but were often located in the villages and therefore easily accessible. Among the formal providers there were 4 times as many private for profit providers than public, 76 versus 18. However, most of the private units were one-person drug shops.In the household survey, 2580 persons were interviewed. 1097 (42%) had experienced illness during the preceding month. Care was sought in 54.1% of the cases. 35.6% were given self-treatment and in 10.3% no action was taken. Of the episodes for which people sought care at a health care facility, 37.0% visited a public health care provider, 39.7% a for profit provider, 11.8% a private not for profit provider, and 10.6% a traditional practitioner. Private for profit facilities were the most popular for ambulatory health care, while public facilities were preferred for more serious conditions and for hospitalization. Traditional practitioners were many but saw relatively few patients. They were mostly used for social problems and limited medical specific conditions.
Conclusions: Private providers play a major role in health care delivery in rural Uganda; reaching a wide client base. Traditional practitioners are many but have as much a social as a medical function in the community. The significance of the private health care sector points to the need to establish a policy that addresses quality and affordability issues and creates a strong regulatory environment for private practice in sub-Saharan Africa.
Figures
References
LinkOut - more resources
Full Text Sources
