

Tumor regression and growth rates determined in five intramural NCI prostate cancer trials: the growth rate constant as an indicator of therapeutic efficacy
- PMID: 21106727
- PMCID: PMC6667189
- DOI: 10.1158/1078-0432.CCR-10-1762
Tumor regression and growth rates determined in five intramural NCI prostate cancer trials: the growth rate constant as an indicator of therapeutic efficacy
Abstract
Purpose: In solid tumors such as prostate cancer, novel paradigms are needed to assess therapeutic efficacy. We utilized a method estimating tumor growth and regression rate constants from serial PSA measurements, and assessed its potential in patients with metastatic castration resistant prostate carcinoma (mCRPC).
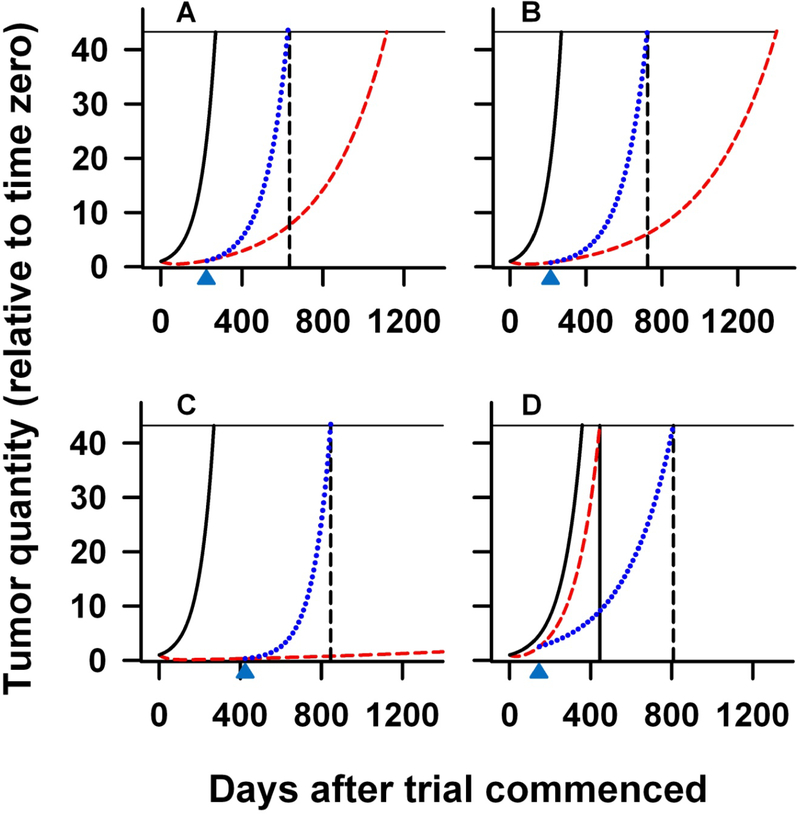
Experimental design: Patients were enrolled in five phase II studies, including an experimental vaccine trial, representing the evolution of therapy in mCRPC. PSA measurements obtained before, and during, therapy were used. Data analysis using a two-phase mathematical equation yielded concomitant PSA growth and regression rate constants.
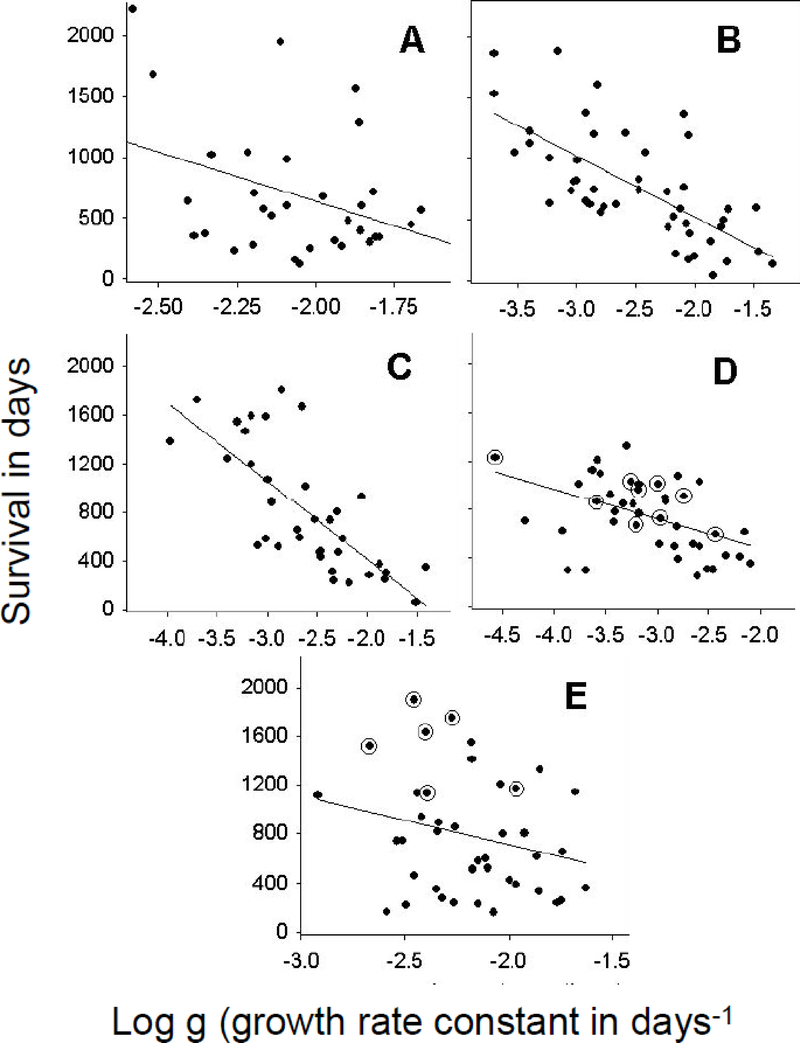
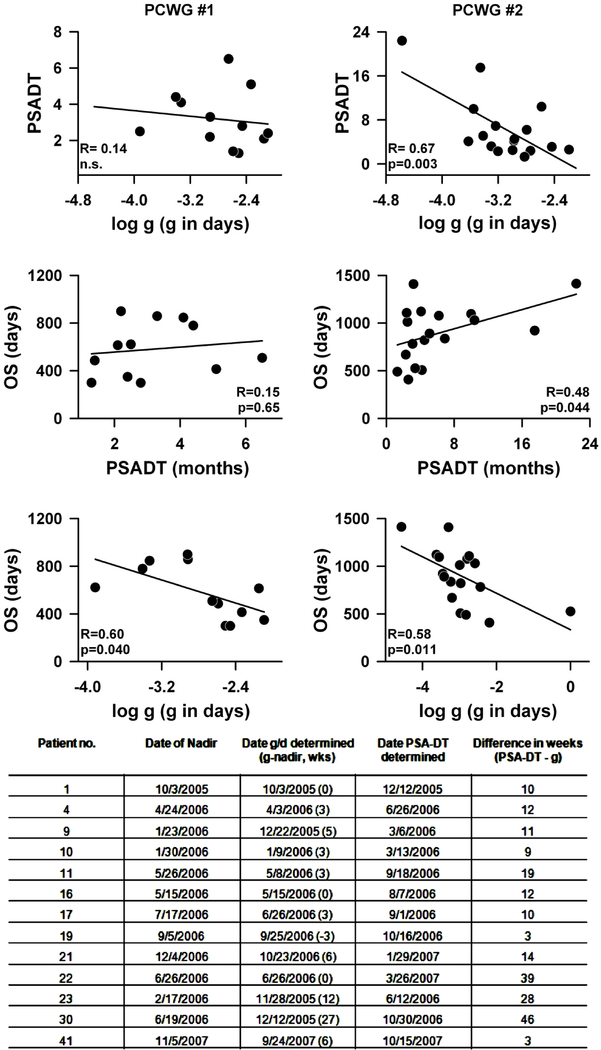
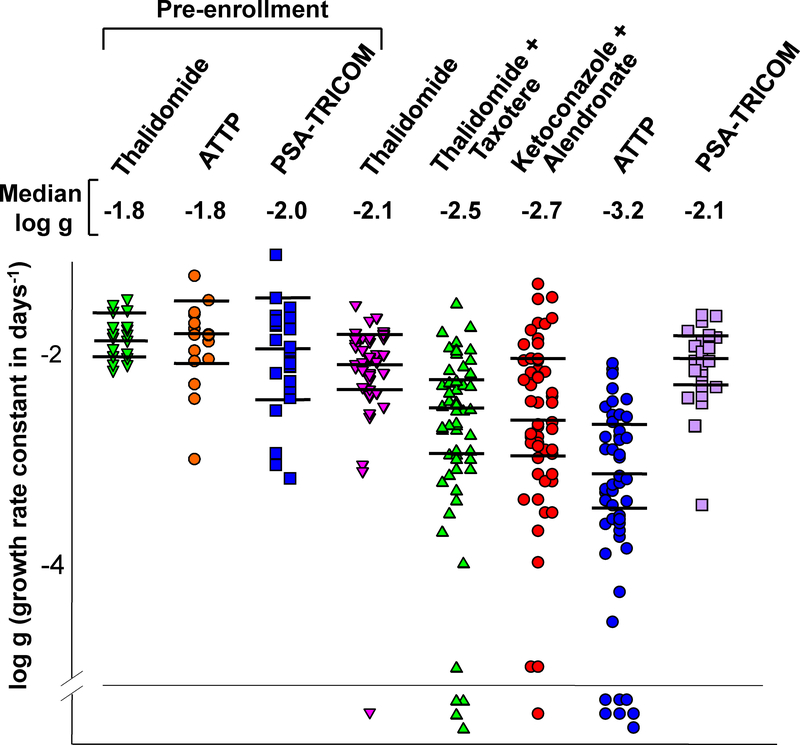
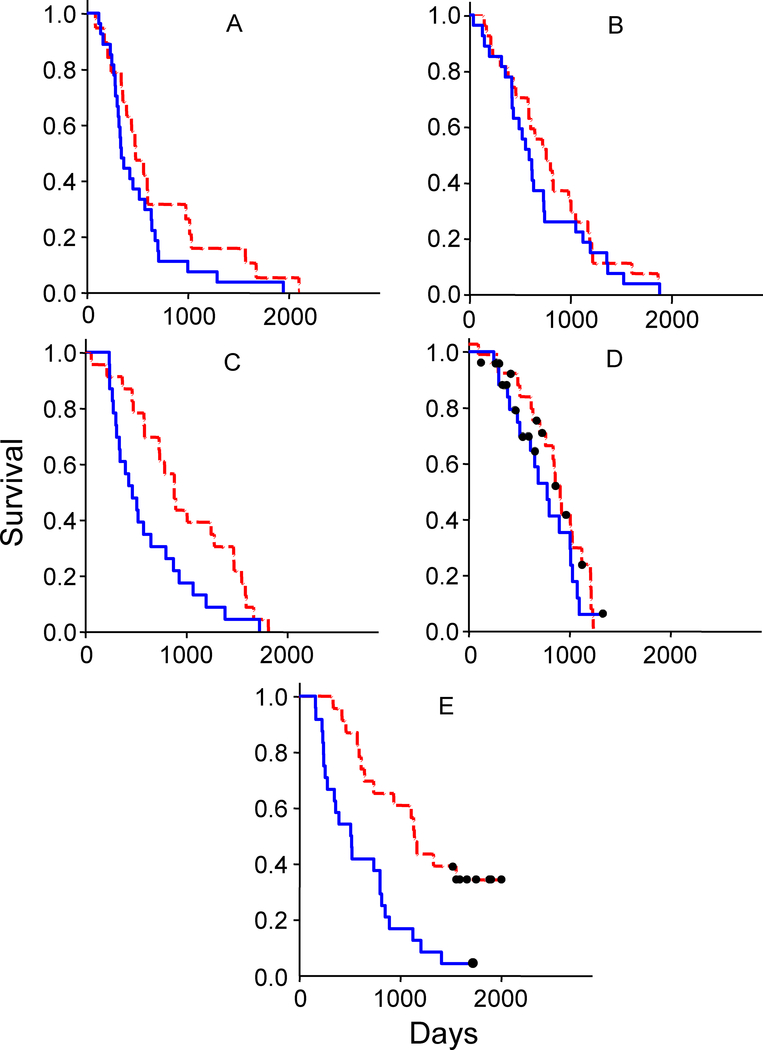
Results: Growth rate constants (g) can be estimated while patients receive therapy and in such patients g is superior to PSA-DT in predicting OS. Incremental reductions in growth rate constants were recorded in successive trials with a 10-fold slower g in the most recent combination therapy trial (log g = 10(-3.17)) relative to single-agent thalidomide (log g = 10(-2.08)) more than a decade earlier. Growth rate constants correlated with survival, except in patients receiving vaccine-based therapy where the evidence demonstrates prolonged survival presumably due to immunity developing subsequent to vaccine administration.
Conclusion: Incremental reductions in tumor growth rate constants suggest increased efficacy in successive chemotherapy trials. The derived growth rate constant correlates with survival, and may be used to assess efficacy. The PSA-TRICOM vaccine appears to have provided marked benefit not apparent during vaccination, but consistent with subsequent development of a beneficial immune response. If validated as a surrogate for survival, growth rate constants would offer an important new efficacy endpoint for clinical trials.
©2010 AACR.
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2009. Atlanta: American Cancer Society; 2009. http://www.cancer.org/docroot/STT/stt_0.asp
-
- Petrylak D Therapeutic options in androgen-independent prostate cancer: building on docetaxel. BJU Int. 2005; 96 Suppl 2:41–6. - PubMed
-
- Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. JAMA. 2005; 294:238–44. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
