

Lumbopelvic alignment on standing lateral radiograph of adult volunteers and the classification in the sagittal alignment of lumbar spine
- PMID: 21107987
- PMCID: PMC3082671
- DOI: 10.1007/s00586-010-1626-0
Lumbopelvic alignment on standing lateral radiograph of adult volunteers and the classification in the sagittal alignment of lumbar spine
Abstract
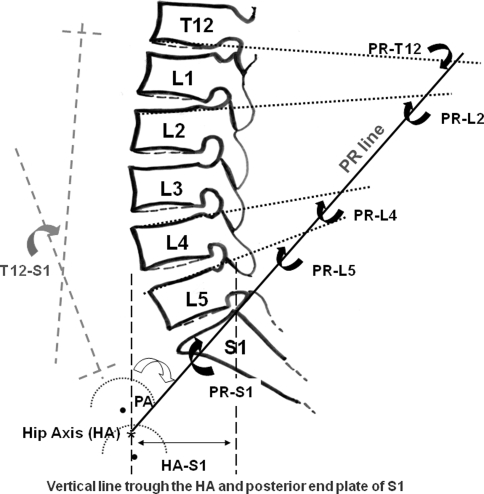
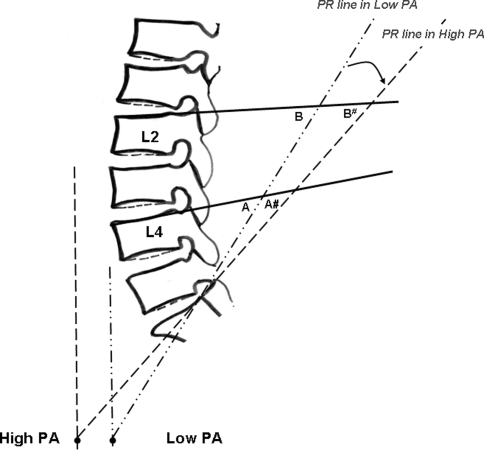
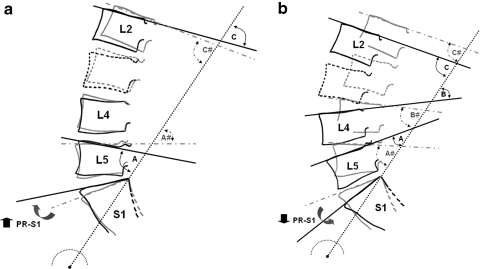
The analysis of the sagittal balance is important for the understanding of the lumbopelvic biomechanics. Results from previous studies documented the correlation between sacro-pelvic orientation and lumbar lordosis and a uniqueness of spino-pelvic alignment in an individual person. This study was subjected to determine the lumbopelvic orientation using pelvic radius measurement technique. The standing lateral radiographs in a standardized standing position were taken from 100 healthy volunteers. The measurements which included hip axis (HA), pelvic radius (PR), pelvic angle (PA), pelvic morphology (PR-S1), sacral translation distance (HA-S1), total lumbosacral lordosis (T12-S1), total lumbopelvic lordosis (PR-T12) and regional lumbopelvic lordosis angles (PR-L2, PR-L4 and PR-L5) were carried out with two independent observers. The relationships between the parameters were as follows. PR-S1 demonstrated positive correlation to regional lumbopelvic lordosis and revealed negative correlation to T12-S1. PA showed negative correlation to PR-S1 and regional lumbopelvic lordosis, but revealed positive correlation to HA-S1. T12-S1 was significantly increased when PR-S1 was lesser than average (35°-45°) and was significantly decreased when PR-S1 was above the average. PR-L4 and PR-L5 were significantly reduced when PR-S1 was smaller than average and only PR-L5 was significantly increased when PR-S1 was above the average. In conclusion, this present study supports that lumbar spine and pelvis work together in order to maintain lumbopelvic balance.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
