

Association between dietary fat content and outcomes in pediatric burn patients
- PMID: 21109263
- PMCID: PMC3419386
- DOI: 10.1016/j.jss.2010.10.006
Association between dietary fat content and outcomes in pediatric burn patients
Abstract
Background: The aim of the study was to compare a low fat/high-carbohydrate diet and a high-fat diet on clinical outcomes by a retrospective cohort study.
Methods: Nine hundred forty-four children with burns ≥ 40% of their total body surface area (TBSA) were divided into two groups: patients receiving Vivonex T.E.N. (low-fat/high-carbohydrate diet; n = 518) and patients receiving milk (high-fat diet; n = 426). Patient demographics, caloric intake, length of hospital stay, and incidence of sepsis, mortality, hepatic steatosis, and organomegaly at autopsy were determined.
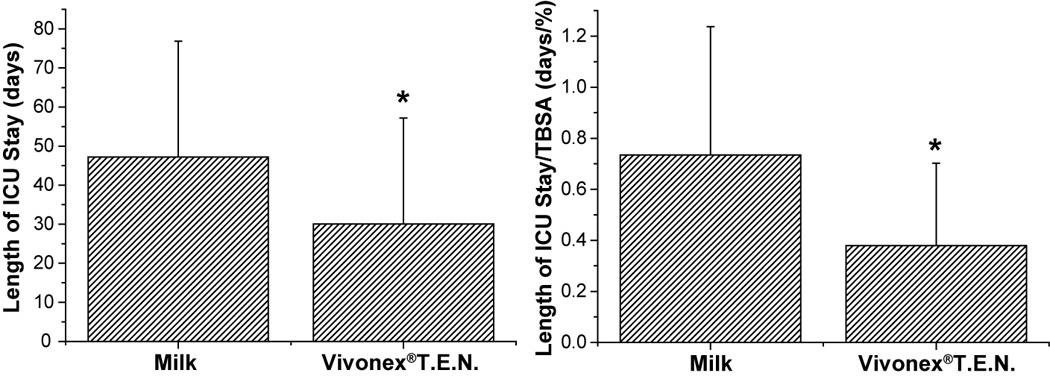
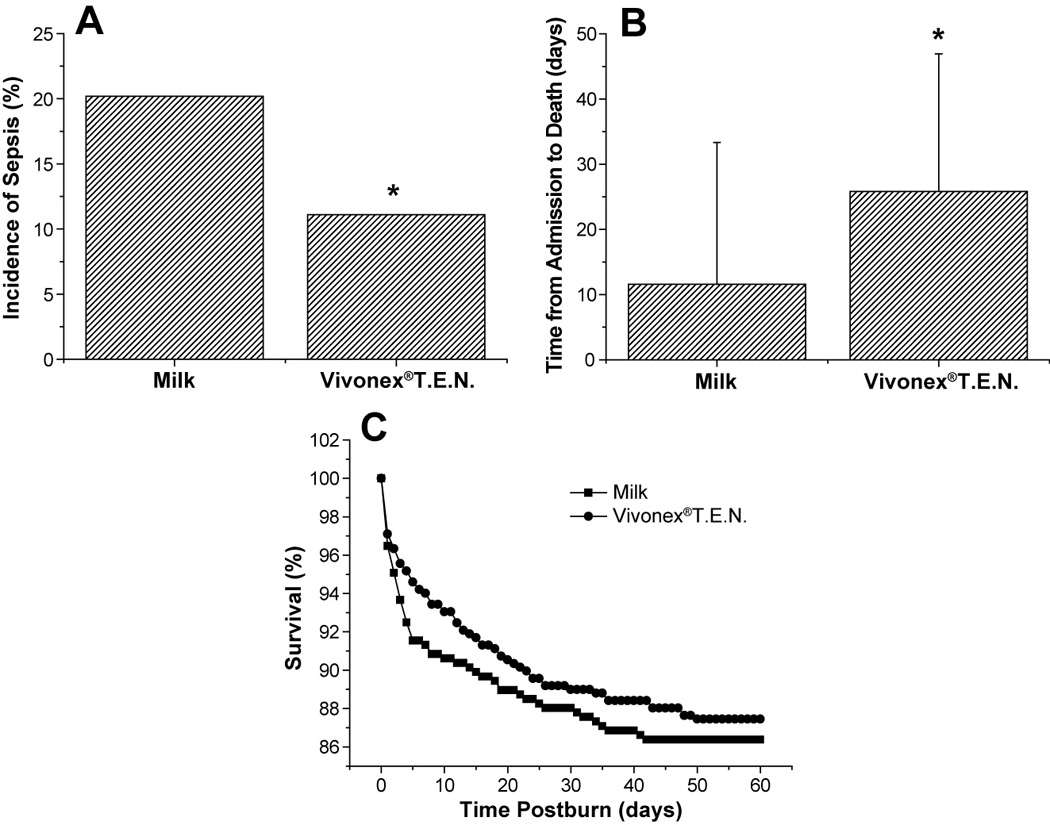
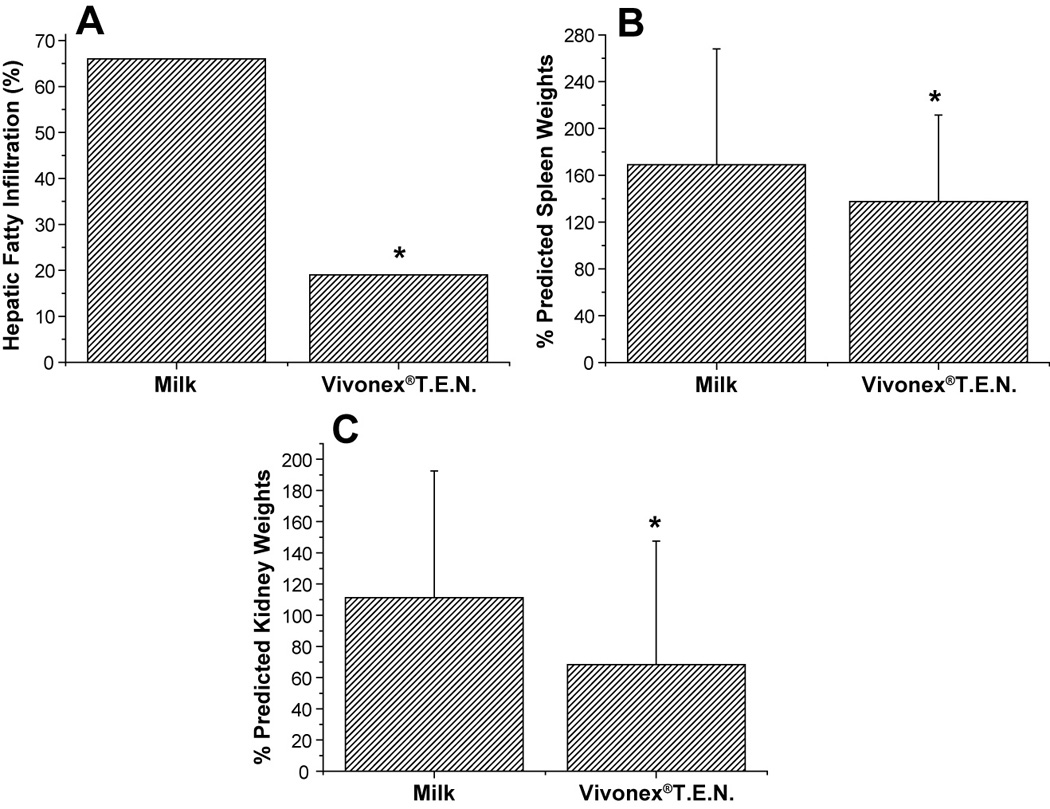
Results: Demographics and caloric intake were similar in both groups. Patients receiving Vivonex T.E.N. had shorter (intensive care unit) ICU stays (Vivonex T.E.N.: 31 ± 2 d; milk: 47 ± 2 d; P < 0.01), shorter ICU stay per % TBSA burn (Vivonex T.E.N.: 0.51 ± 0.02 d/%; milk: 0.77 ± 0.03 d/%; P < 0.01), lower incidence of sepsis (Vivonex T.E.N.: 11%; milk: 20%; P < 0.01), and lived significantly longer until death than those receiving milk (Vivonex T.E.N.: 20 ± 3 d; milk: 10 ± 2 d; P < 0.01). There was no difference in overall mortality between the two groups (Vivonex T.E.N.:15% versus milk: 13%; P < 0.9). Autopsies revealed decreased hepatic steatosis and decreased enlargement of kidney and spleen in patients receiving Vivonex T.E.N.
Conclusions: The period with a low-fat/high-carbohydrate diet was associated with lower LOS, decreased incidence of organomegaly, infection, and hepatic steatosis post-burn compared with the period when a high-fat diet was used. These associations indicate the benefit of high carbohydrate/low fat nutrition; however, the findings in these time periods can also be likely due to the multifactorial effects of advances in burn care. We believe that these results have some relevance because high fat is associated with poorer outcomes compared with low fat.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Geometric framework reveals that a moderate protein, high carbohydrate intake is optimal for severe burn injury in mice.Br J Nutr. 2020 May 14;123(9):1056-1067. doi: 10.1017/S0007114520000276. Epub 2020 Jan 27. Br J Nutr. 2020. PMID: 31983360
-
Nutritional hepatic steatosis and mortality after burn injury in rats.Clin Nutr. 1998 Dec;17(6):293-9. doi: 10.1016/s0261-5614(98)80322-1. Clin Nutr. 1998. PMID: 10205353
-
Clinical outcomes after burns in elderly patients over 70 years: A 17-year retrospective analysis.Burns. 2018 Feb;44(1):65-69. doi: 10.1016/j.burns.2017.09.018. Epub 2017 Oct 20. Burns. 2018. PMID: 29066003
-
High-Carbohydrate vs High-Fat Nutrition for Burn Patients.Nutr Clin Pract. 2019 Oct;34(5):688-694. doi: 10.1002/ncp.10396. Epub 2019 Aug 22. Nutr Clin Pract. 2019. PMID: 31441112 Review.
-
Nutrition in infancy and childhood.Prim Care. 1982 Sep;9(3):497-516. Prim Care. 1982. PMID: 6755518 Review. No abstract available.
Cited by
-
Metabolic and Hormonal Changes in Pediatric Burn Patients: Mechanisms, Evidence, and Care Strategies.Eur Burn J. 2025 Apr 7;6(2):17. doi: 10.3390/ebj6020017. Eur Burn J. 2025. PMID: 40265372 Free PMC article. Review.
-
35ème congrès SFB, table ronde «nutrition»: transcription des communications.Ann Burns Fire Disasters. 2015 Dec 31;28(4):296-309. Ann Burns Fire Disasters. 2015. PMID: 27777551 Free PMC article. French.
-
Effects of Different Ratios of Carbohydrate-Fat in Enteral Nutrition on Metabolic Pattern and Organ Damage in Burned Rats.Nutrients. 2022 Sep 4;14(17):3653. doi: 10.3390/nu14173653. Nutrients. 2022. PMID: 36079913 Free PMC article.
-
[Expert consensus on enteral nutrition treatment for burned children (2025 edition)].Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2025 Aug 20;41(8):725-733. doi: 10.3760/cma.j.cn501225-20250206-00054. Zhonghua Shao Shang Yu Chuang Mian Xiu Fu Za Zhi. 2025. PMID: 40850817 Free PMC article. Chinese.
-
The Emerging Therapeutic Role of Medical Foods for Gastrointestinal Disorders.Gastroenterol Hepatol (N Y). 2017 Feb;13(2):104-115. Gastroenterol Hepatol (N Y). 2017. PMID: 28450817 Free PMC article.
References
-
- Wolfe RR, Herndon DN, Jahoor F, et al. Effect of severe burn injury on substrate cycling by glucose and fatty acids. N Engl J Med. 1987;317:403. - PubMed
-
- Herndon DN, Tompkins RG. Support of the metabolic response to burn injury. Lancet. 2004;363:1895. - PubMed
-
- Demling RH, Seigne P. Metabolic management of patients with severe burns. World J Surg. 2000;24:673. - PubMed
-
- Herndon DN, Hart DW, Wolf SE, et al. Reversal of catabolism by beta-blockade after severe burns. N Engl J Med. 2001;345:1223. - PubMed
-
- Saffle JR, Graves C. Nutritional support of the burned patient. In: Herndon DN, editor. Total Burn Care. London: Saunders; 2007. p. 398.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
