

Investigation of anal motor characteristics of the sensorimotor response (SMR) using 3-D anorectal pressure topography
- PMID: 21109594
- PMCID: PMC3043653
- DOI: 10.1152/ajpgi.00348.2010
Investigation of anal motor characteristics of the sensorimotor response (SMR) using 3-D anorectal pressure topography
Abstract
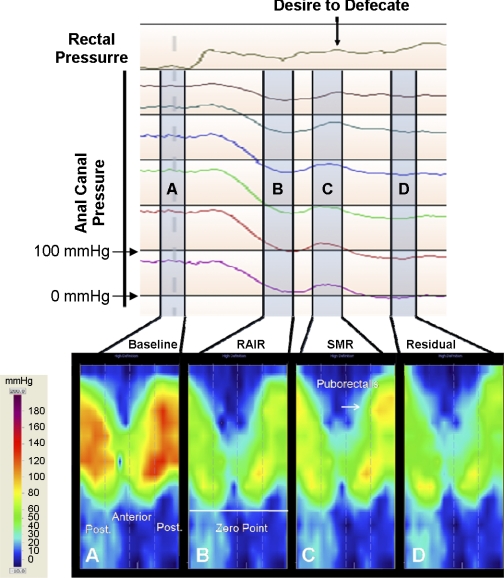
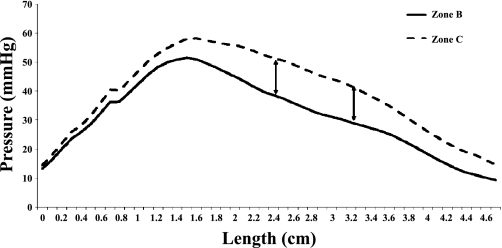
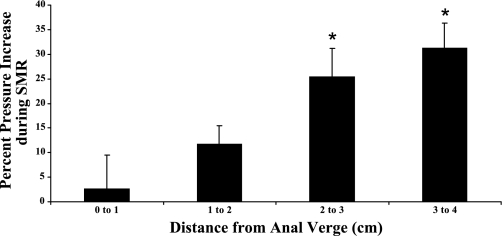
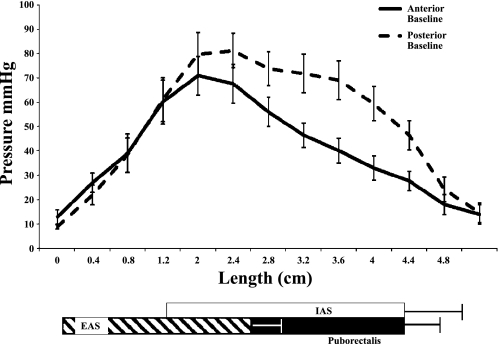
Desire to defecate is associated with a unique anal contractile response, the sensorimotor response (SMR). However, the precise muscle(s) involved is not known. We aimed to examine the role of external and internal anal sphincter and the puborectalis muscle in the genesis of SMR. Anorectal 3-D pressure topography was performed in 10 healthy subjects during graded rectal balloon distention using a novel high-definition manometry system consisting of a probe with 256 pressure sensors arranged circumferentially. The anal pressure changes before, during, and after the onset of SMR were measured at every millimeter along the length of anal canal and in 3-D by dividing the anal canal into 4 × 2.1-mm grids. Pressures were assessed in the longitudinal and anterior-posterior axis. Anal ultrasound was performed to assess puborectalis morphology. 3-D topography demonstrated that rectal distention produced an SMR coinciding with desire to defecate and predominantly induced by contraction of puborectalis. Anal ultrasound showed that the puborectalis was located at mean distance of 3.5 cm from anal verge, which corresponded with peak pressure difference between the anterior and posterior vectors observed at 3.4 cm with 3-D topography (r = 0.77). The highest absolute and percentage increases in pressure during SMR were seen in the superior-posterior portion of anal canal, reaffirming the role of puborectalis. The SMR anal pressure profile showed a peak pressure at 1.6 cm from anal verge in the anterior and posterior vectors and distinct increase in pressure only posteriorly at 3.2 cm corresponding to puborectalis. We concluded that SMR is primarily induced by the activation and contraction of the puborectalis muscle in response to a sensation of a desire to defecate.
Figures
Similar articles
-
Topographic and manometric characterization of the recto-anal inhibitory reflex.Neurogastroenterol Motil. 2012 Mar;24(3):e147-54. doi: 10.1111/j.1365-2982.2011.01857.x. Epub 2012 Jan 11. Neurogastroenterol Motil. 2012. PMID: 22235880 Free PMC article.
-
[Morphological characteristic of anal canal in patients with dyssynergic defecation and its correlation with anorectal manometry].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 May 25;22(5):457-463. doi: 10.3760/cma.j.issn.1671-0274.2019.05.012. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31104432 Chinese.
-
Rectoanal sensorimotor response in humans during rectal distension.Dis Colon Rectum. 2007 Oct;50(10):1639-46. doi: 10.1007/s10350-007-0257-y. Dis Colon Rectum. 2007. PMID: 17762970
-
High resolution and high definition anorectal manometry and pressure topography: diagnostic advance or a new kid on the block?Curr Gastroenterol Rep. 2013 Dec;15(12):360. doi: 10.1007/s11894-013-0360-2. Curr Gastroenterol Rep. 2013. PMID: 24271955 Review.
-
[Anorectal functional study. The state of the art].Minerva Chir. 1994 Dec;49(12):1187-93. Minerva Chir. 1994. PMID: 7746437 Review. Italian.
Cited by
-
Accuracy and Reproducibility of High-definition Anorectal Manometry and Pressure Topography Analyses in Healthy Subjects.Clin Gastroenterol Hepatol. 2015 Jun;13(6):1143-50.e1. doi: 10.1016/j.cgh.2014.12.034. Epub 2015 Jan 20. Clin Gastroenterol Hepatol. 2015. PMID: 25616028 Free PMC article.
-
Purse-string morphology of external anal sphincter revealed by novel imaging techniques.Am J Physiol Gastrointest Liver Physiol. 2014 Mar;306(6):G505-14. doi: 10.1152/ajpgi.00338.2013. Epub 2014 Jan 23. Am J Physiol Gastrointest Liver Physiol. 2014. PMID: 24458022 Free PMC article.
-
Short and long term results of anatomical reconstruction of perineal body and sphincter complex in obstetric anal sphincter injuries.Turk J Surg. 2022 Jun 29;38(2):159-168. doi: 10.47717/turkjsurg.2022.5528. eCollection 2022 Jun. Turk J Surg. 2022. PMID: 36483166 Free PMC article.
-
Three-dimension High-resolution Anorectal Manometry Can Precisely Measure Perineal Descent.J Neurogastroenterol Motil. 2013 Apr;19(2):257-8. doi: 10.5056/jnm.2013.19.2.257. Epub 2013 Apr 16. J Neurogastroenterol Motil. 2013. PMID: 23667758 Free PMC article. No abstract available.
-
Is the extent of obstetric anal sphincter injury correlated with the severity of fecal incontinence in the long term?Tech Coloproctol. 2020 Jan;24(1):49-55. doi: 10.1007/s10151-019-02128-1. Epub 2019 Dec 9. Tech Coloproctol. 2020. PMID: 31820190
References
-
- Beuret-Blanquart F, Weber J, Gouverneur JP, Demangeon S, Denis P. Colonic transit time and anorectal manometric anomalies in 19 patients with complete transection of the spinal cord. J Auton Nerv Syst 30: 199–207, 1990 - PubMed
-
- Bharucha AE. Pelvic floor: anatomy and function. Neurogastroenterol Motil 18: 507–519, 2006 - PubMed
-
- Cornella JL, Hibner M, Fenner DE, Kriegshauser JS, Hentz J, Magrina JF. Three-dimensional reconstruction of magnetic resonance images of the anal sphincter and correlation between sphincter volume and pressure. Am J Obstet Gynecol 189: 130–135, 2003 - PubMed
-
- Cortesini C, Pucciani F, Carassale GL, Paparozzi C. Anorectal physiology after anterior resection and pull-through operation. Eur Surg Res 15: 176–183, 1983 - PubMed
-
- De Ocampo S, Remes-Troche JM, Miller MJ, Rao SSC. Rectoanal sensorimotor response in humans during rectal distension. Dis Colon Rectum 50: 1639–1646, 2007 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical