

Improved cardiovascular diagnostic accuracy by pocket size imaging device in non-cardiologic outpatients: the NaUSiCa (Naples Ultrasound Stethoscope in Cardiology) study
- PMID: 21110840
- PMCID: PMC3003628
- DOI: 10.1186/1476-7120-8-51
Improved cardiovascular diagnostic accuracy by pocket size imaging device in non-cardiologic outpatients: the NaUSiCa (Naples Ultrasound Stethoscope in Cardiology) study
Abstract
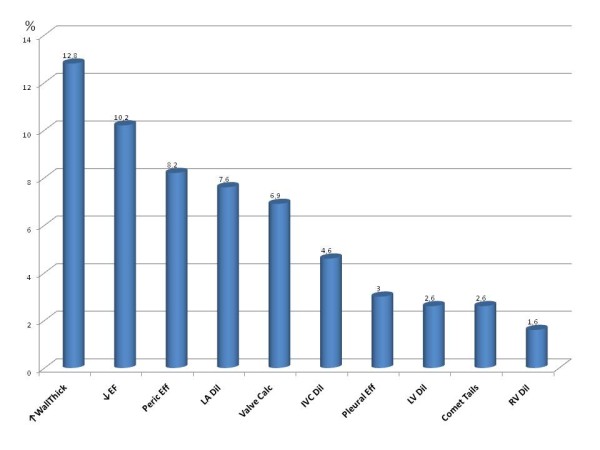
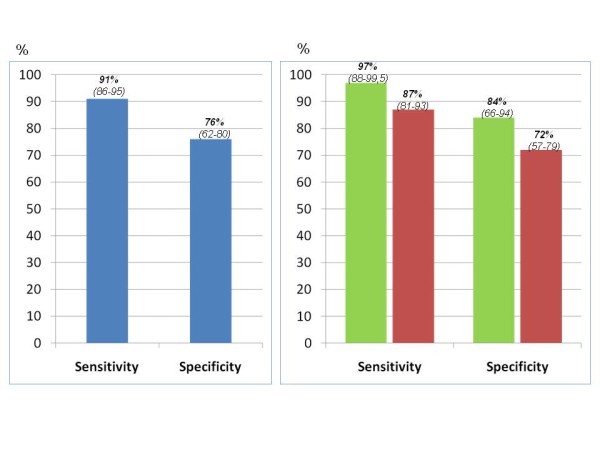
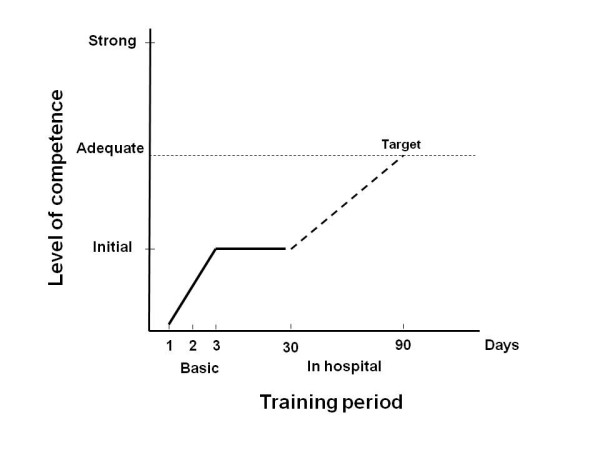
Miniaturization has evolved in the creation of a pocket-size imaging device which can be utilized as an ultrasound stethoscope. This study assessed the additional diagnostic power of pocket size device by both experts operators and trainees in comparison with physical examination and its appropriateness of use in comparison with standard echo machine in a non-cardiologic population. Three hundred four consecutive non cardiologic outpatients underwent a sequential assessment including physical examination, pocket size imaging device and standard Doppler-echo exam. Pocket size device was used by both expert operators and trainees (who received specific training before the beginning of the study). All the operators were requested to give only visual, qualitative insights on specific issues. All standard Doppler-echo exams were performed by expert operators. One hundred two pocket size device exams were performed by experts and two hundred two by trainees. The time duration of the pocket size device exam was 304 ± 117 sec. Diagnosis of cardiac abnormalities was made in 38.2% of cases by physical examination and in 69.7% of cases by physical examination + pocket size device (additional diagnostic power = 31.5%, p < 0.0001). The overall K between pocket size device and standard Doppler-echo was 0.67 in the pooled population (0.84 by experts and 0.58 by trainees). K was suboptimal for trainees in the eyeball evaluation of ejection fraction, left atrial dilation and right ventricular dilation. Overall sensitivity was 91% and specificity 76%. Sensitivity and specificity were lower in trainees than in experts. In conclusion, pocket size device showed a relevant additional diagnostic value in comparison with physical examination. Sensitivity and specificity were good in experts and suboptimal in trainees. Specificity was particularly influenced by the level of experience. Training programs are needed for pocket size device users.
Figures
References
-
- Seward JB, Douglas PS, Erbel R, Kerber RE, Kronzon I, Rakowski H, Sahn DJ, Sisk EJ, Tajik AJ, Wann S. Hand-carried cardiac ultrasound (HCU) device: Recommendations regarding new technology. A report from the Echocardiography Task Force on new technology of the nomenclature and Standard Committee of the American Society of Echocardiography. J Am Soc Echocardiogr. 2002;15:369–373. doi: 10.1067/mje.2002.123026. - DOI - PubMed
-
- Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise J, Solomon S, Spencer KT, St John Sutton M, Stewart W. American Society of Echocardiography's Nomenclature and Standards Committee; Task Force on Chamber Quantification; American College of Cardiology Echocardiography Committee; American Heart Association; European Association of Echocardiography, European Society of Cardiology. Eur J Echocardiogr. 2006;7:79–108. doi: 10.1016/j.euje.2005.12.014. - DOI - PubMed
-
- Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flaschskampf A, Pellika PA, Evangelista A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009;10:165–193. doi: 10.1093/ejechocard/jep007. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
