

No agreement of mixed venous and central venous saturation in sepsis, independent of sepsis origin
- PMID: 21114844
- PMCID: PMC3219992
- DOI: 10.1186/cc9348
No agreement of mixed venous and central venous saturation in sepsis, independent of sepsis origin
Abstract
Introduction: Controversy remains regarding the relationship between central venous saturation (ScvO(2)) and mixed venous saturation (SvO(2)) and their use and interchangeability in patients with sepsis or septic shock. We tested the hypothesis that ScvO(2) does not reliably predict SvO(2) in sepsis. Additionally we looked at the influence of the source (splanchnic or non-splanchnic) of sepsis on this relationship.
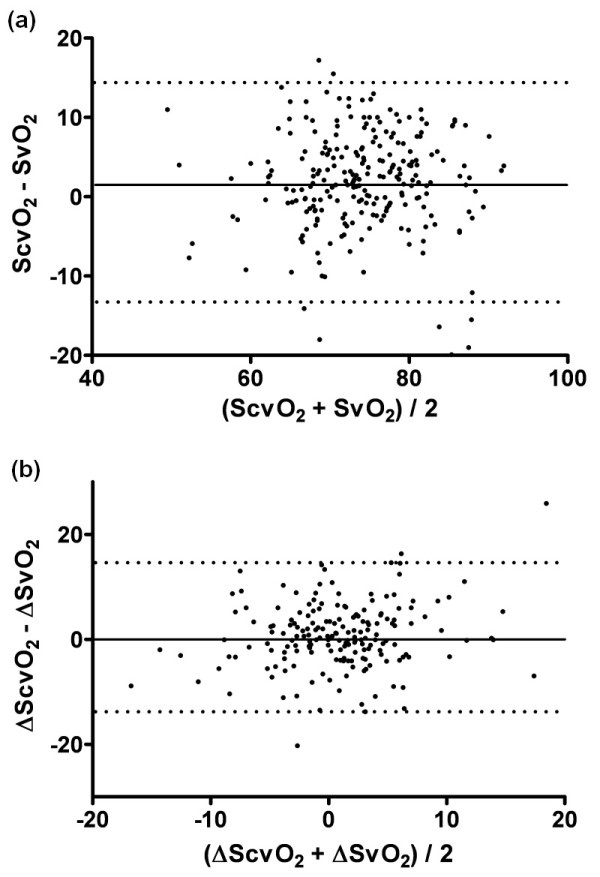
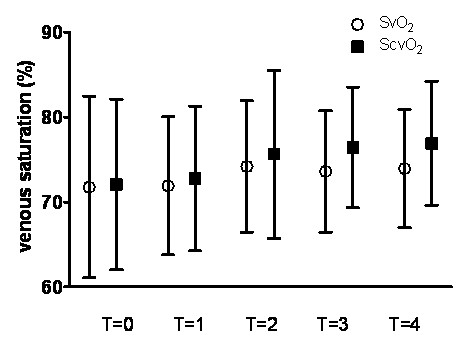
Methods: In this prospective observational two-center study we concurrently determined ScvO(2) and SvO(2) in a group of 53 patients with severe sepsis during the first 24 hours after admission to the intensive care units in 2 Dutch hospitals. We assessed correlation and agreement of ScvO(2) and SvO(2), including the difference, i.e. the gradient, between ScvO(2) and SvO(2) (ScvO(2) - SvO(2)). Additionally, we compared the mean differences between ScvO(2) and SvO(2) of both splanchnic and non-splanchnic group.
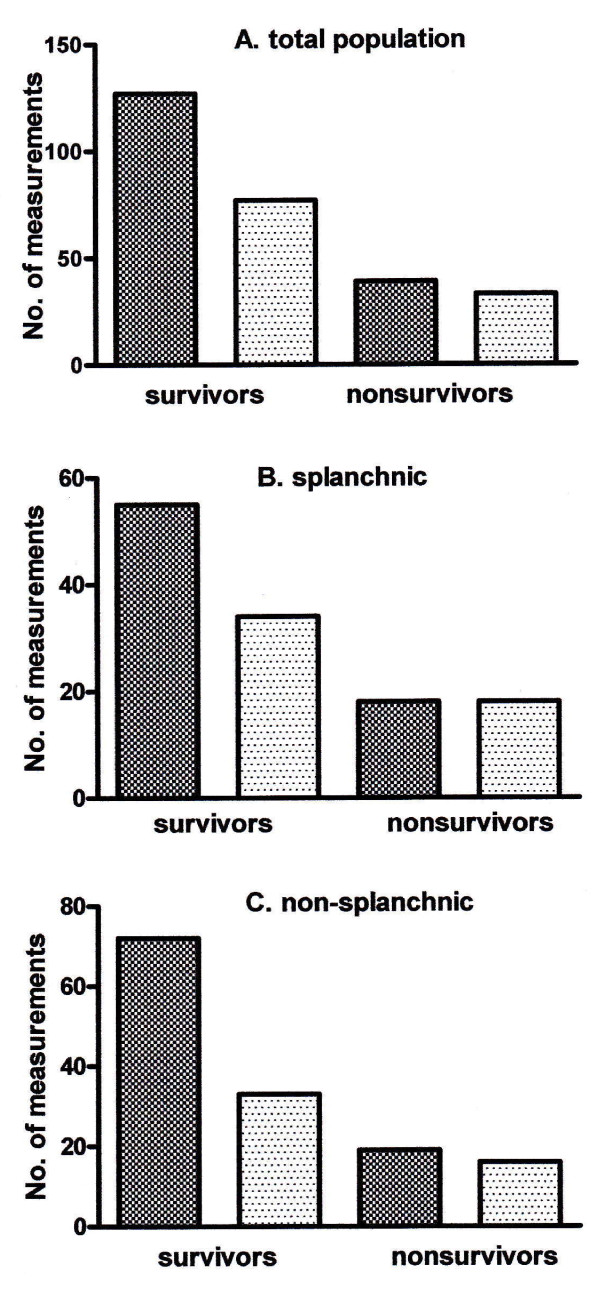
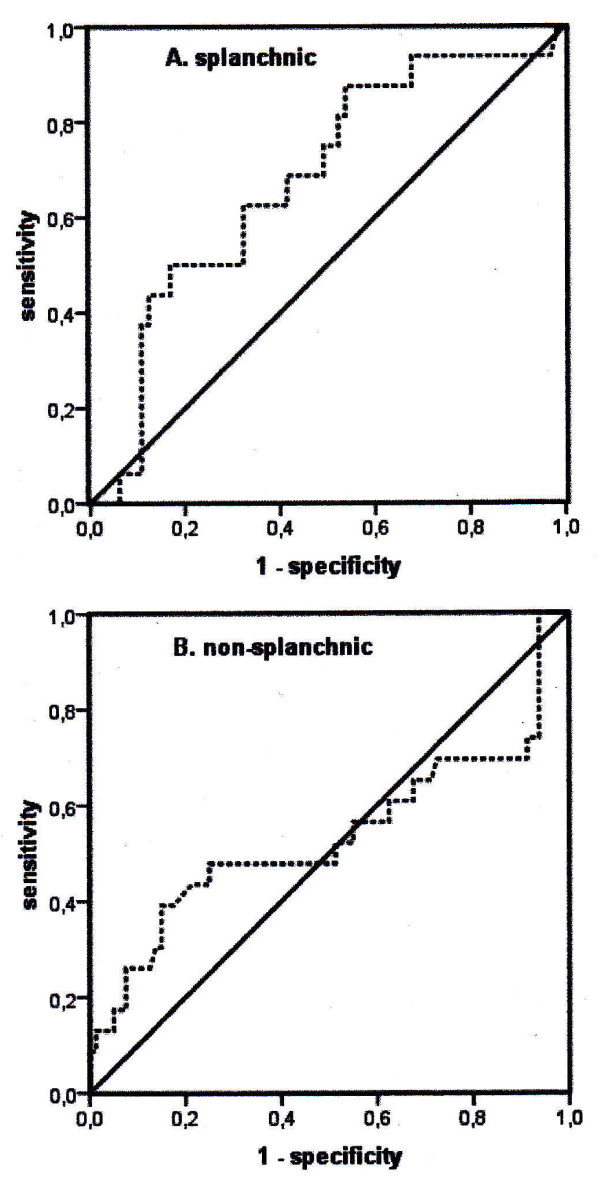
Results: A total of 265 paired blood samples were obtained. ScvO(2) overestimated SvO(2) by less than 5% with wide limits of agreement. For changes in ScvO(2) and SvO(2) results were similar. The distribution of the (ScvO(2) - SvO(2)) (< 0 or ≥ 0) was similar in survivors and nonsurvivors. The mean (ScvO(2) - SvO(2)) in the splanchnic group was similar to the mean (ScvO(2) - SvO(2)) in the non-splanchnic group (0.8 ± 3.9% vs. 2.5 ± 6.2%; P = 0.30). O(2)ER (P = 0.23) and its predictive value for outcome (P = 0.20) were similar in both groups.
Conclusions: ScvO(2) does not reliably predict SvO(2) in patients with severe sepsis. The trend of ScvO(2) is not superior to the absolute value in this context. A positive difference (ScvO(2) - SvO(2)) is not associated with improved outcome.
Figures
Comment in
-
ICU survival and the central to mixed venous oxygen difference.Crit Care. 2011;15(3):436; author reply 436. doi: 10.1186/cc10260. Epub 2011 Jun 30. Crit Care. 2011. PMID: 21722335 Free PMC article. No abstract available.
References
-
- Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall J, Parker MM, Ramsay G, Zimmerman JL, Vincent JL, Levy MM. for Surviving Sepsis Campaign. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858–873. doi: 10.1097/01.CCM.0000117317.18092.E4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
