

Klotho deficiency causes vascular calcification in chronic kidney disease
- PMID: 21115613
- PMCID: PMC3014041
- DOI: 10.1681/ASN.2009121311
Klotho deficiency causes vascular calcification in chronic kidney disease
Abstract
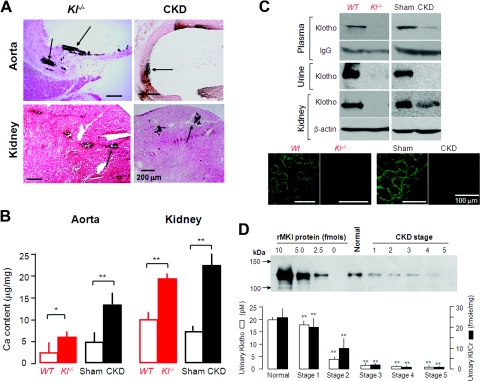
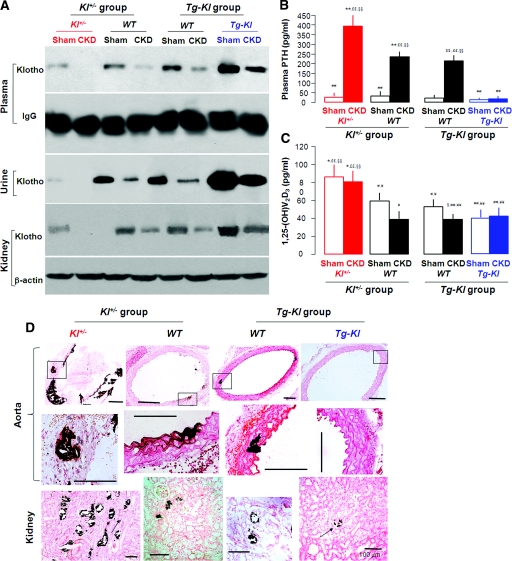
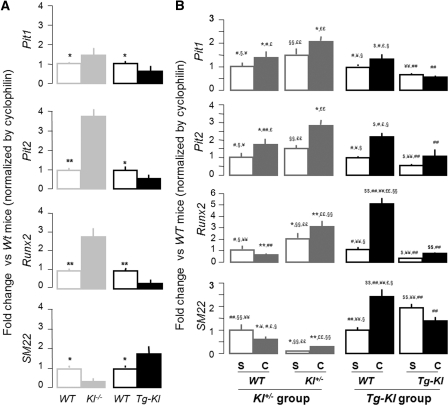
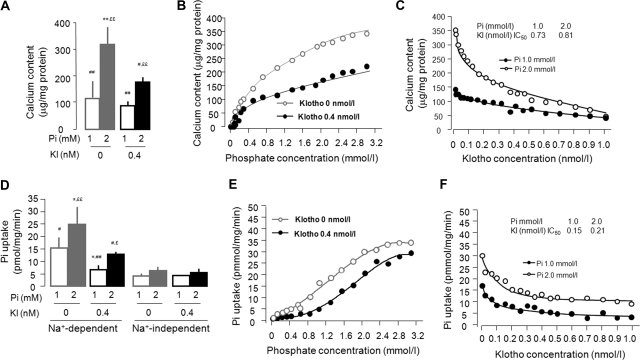
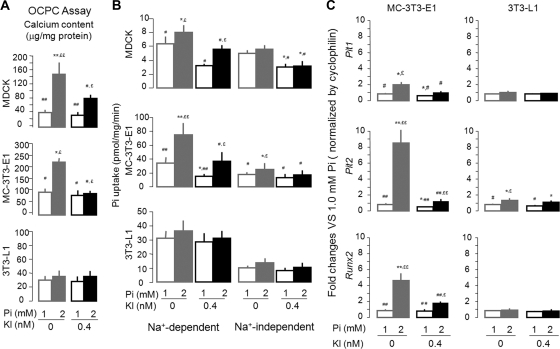
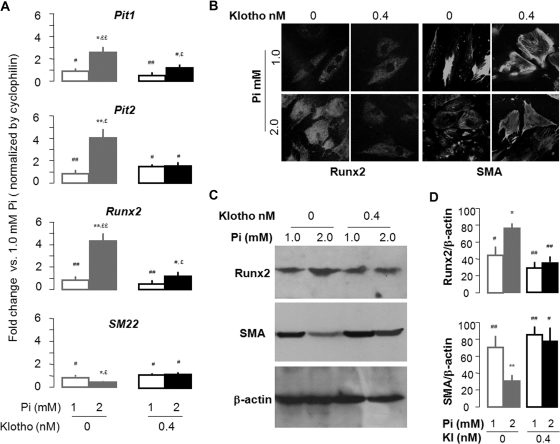
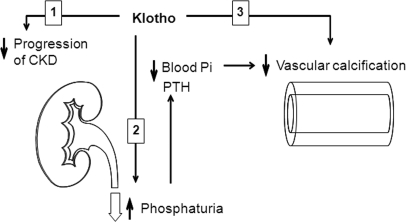
Soft-tissue calcification is a prominent feature in both chronic kidney disease (CKD) and experimental Klotho deficiency, but whether Klotho deficiency is responsible for the calcification in CKD is unknown. Here, wild-type mice with CKD had very low renal, plasma, and urinary levels of Klotho. In humans, we observed a graded reduction in urinary Klotho starting at an early stage of CKD and progressing with loss of renal function. Despite induction of CKD, transgenic mice that overexpressed Klotho had preserved levels of Klotho, enhanced phosphaturia, better renal function, and much less calcification compared with wild-type mice with CKD. Conversely, Klotho-haploinsufficient mice with CKD had undetectable levels of Klotho, worse renal function, and severe calcification. The beneficial effect of Klotho on vascular calcification was a result of more than its effect on renal function and phosphatemia, suggesting a direct effect of Klotho on the vasculature. In vitro, Klotho suppressed Na(+)-dependent uptake of phosphate and mineralization induced by high phosphate and preserved differentiation in vascular smooth muscle cells. In summary, Klotho is an early biomarker for CKD, and Klotho deficiency contributes to soft-tissue calcification in CKD. Klotho ameliorates vascular calcification by enhancing phosphaturia, preserving glomerular filtration, and directly inhibiting phosphate uptake by vascular smooth muscle. Replacement of Klotho may have therapeutic potential for CKD.
Figures

Comment in
-
Klotho: an elixir of youth for the vasculature?J Am Soc Nephrol. 2011 Jan;22(1):5-7. doi: 10.1681/ASN.2010111190. Epub 2010 Dec 16. J Am Soc Nephrol. 2011. PMID: 21164022 No abstract available.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Mizobuchi M, Towler D, Slatopolsky E: Vascular calcification: The killer of patients with chronic kidney disease. J Am Soc Nephrol 20: 1453–1464, 2009 - PubMed
-
- Baber U, de Lemos JA, Khera A, McGuire DK, Omland T, Toto RD, Hedayati SS: Non-traditional risk factors predict coronary calcification in chronic kidney disease in a population-based cohort. Kidney Int 73: 615–621, 2008 - PubMed
-
- Wallin R, Wajih N, Greenwood GT, Sane DC: Arterial calcification: A review of mechanisms, animal models, and the prospects for therapy. Med Res Rev 21: 274–301, 2001 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
