

Association of chronic kidney disease with muscle deficits in children
- PMID: 21115614
- PMCID: PMC3029910
- DOI: 10.1681/ASN.2010060603
Association of chronic kidney disease with muscle deficits in children
Abstract
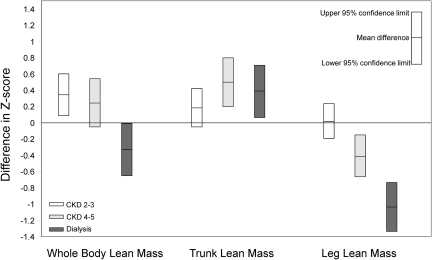
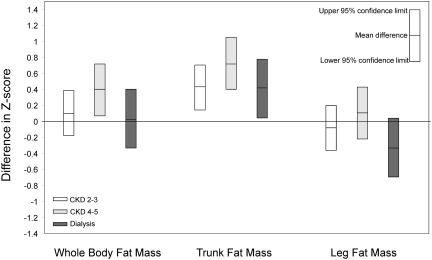
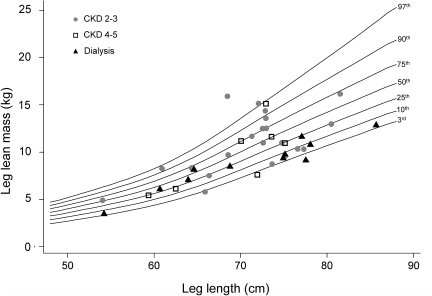
The effect of chronic kidney disease (CKD) on muscle mass in children, independent of poor growth and delayed maturation, is not well understood. We sought to characterize whole body and regional lean mass (LM) and fat mass (FM) in children and adolescents with CKD and to identify correlates of LM deficits in CKD. We estimated LM and FM from dual energy x-ray absorptiometry scans in 143 children with CKD and 958 controls at two pediatric centers. We expressed whole body, trunk, and leg values of LM and FM as Z-scores relative to height, sitting height, and leg length, respectively, using the controls as the reference. We used multivariable regression models to compare Z-scores in CKD and controls, adjusted for age and maturation, and to identify correlates of LM Z-scores in CKD. Greater CKD severity associated with greater leg LM deficits. Compared with controls, leg LM Z-scores were similar in CKD stages 2 to 3 (difference: 0.02 [95% CI: -0.20, 0.24]; P = 0.8), but were lower in CKD stages 4 to 5 (-0.41 [-0.66, -0.15]; P = 0.002) and dialysis (-1.03 [-1.33, -0.74]; P < 0.0001). Among CKD participants, growth hormone therapy associated with greater leg LM Z-score (0.58 [0.03, 1.13]; P = 0.04), adjusted for CKD severity. Serum albumin, bicarbonate, and markers of inflammation did not associate with LM Z-scores. CKD associated with greater trunk LM and FM, variable whole body LM, and normal leg FM, compared with controls. In conclusion, advanced CKD associates with significant deficits in leg lean mass, indicating skeletal muscle wasting. These data call for prospective studies of interventions to improve muscle mass among children with CKD.
Figures
References
-
- Kalantar-Zadeh K, Abbott KC, Salahudeen AK, Kilpatrick RD, Horwich TB: Survival advantages of obesity in dialysis patients. Am J Clin Nutr 81: 543–554, 2005 - PubMed
-
- Kalantar-Zadeh K, Kuwae N, Wu DY, Shantouf RS, Fouque D, Anker SD, Block G, Kopple JD: Associations of body fat and its changes over time with quality of life and prospective mortality in hemodialysis patients. Am J Clin Nutr 83: 202–210, 2006 - PubMed
-
- Leavey SF, Strawderman RL, Jones CA, Port FK, Held PJ: Simple nutritional indicators as independent predictors of mortality in hemodialysis patients. Am J Kidney Dis 31: 997–1006, 1998 - PubMed
-
- Wong CS, Gipson DS, Gillen DL, Emerson S, Koepsell T, Sherrard DJ, Watkins SL, Stehman-Breen C: Anthropometric measures and risk of death in children with end-stage renal disease. Am J Kidney Dis 36: 811–819, 2000 - PubMed
-
- O'Sullivan AJ, Lawson JA, Chan M, Kelly JJ: Body composition and energy metabolism in chronic renal insufficiency. Am J Kidney Dis 39: 369–375, 2002 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
