

Outcomes of active surveillance for men with intermediate-risk prostate cancer
- PMID: 21115873
- PMCID: PMC3058278
- DOI: 10.1200/JCO.2010.31.4252
Outcomes of active surveillance for men with intermediate-risk prostate cancer
Abstract
Purpose: Active surveillance (AS) is an option for the initial management of early-stage prostate cancer. Current risk stratification schema identify patients with low-risk disease who are presumed to be most suitable for AS. However, some men with higher risk disease also elect AS; outcomes for such men have not been widely reported.
Patients and methods: Men managed with AS at University of California, San Francisco, were classified as low- or intermediate-risk based on serum prostate-specific antigen (PSA), Gleason grade, extent of biopsy involvement, and T stage. Clinical and demographic characteristics, and progression in terms of Gleason score, PSA kinetics, and active treatment were compared between men with low- and intermediate-risk tumors.
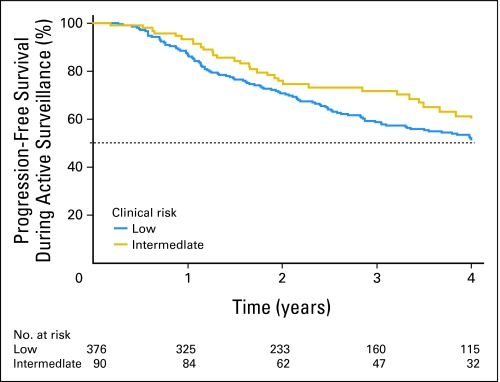
Results: Compared to men with low-risk tumors, those with intermediate-risk tumors were older (mean, 64.9 v 62.3 years) with higher mean PSA values (10.9 v 5.1 ng/mL), and more tumor involvement (mean, 20.4% v 15.3% positive biopsy cores; all P < .01). Within 4 years of the first positive biopsy, the clinical risk group did not differ in terms of the proportions experiencing progression-free survival, (low [54%] v intermediate [61%]; log-rank P = .22) or the proportions who underwent active treatment (low [30%] v intermediate [35%]; log-rank P = .88). Among men undergoing surgery, none were node positive and none had biochemical recurrence within 3 years.
Conclusion: Selected men with intermediate-risk features be appropriate candidates for AS, and are not necessarily more likely to progress. AS for these men may provide an opportunity to further reduce overtreatment of disease that is unlikely to progress to advanced cancer.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Esserman L, Shieh Y, Thompson I. Rethinking screening for breast cancer and prostate cancer. JAMA. 2009;302:1685–1692. - PubMed
-
- Dall'Era MA, Cooperberg MR, Chan JM, et al. Active surveillance for early-stage prostate cancer: Review of the current literature. Cancer. 2008;112:1650–1659. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
