

Recurrence and mortality according to estrogen receptor status for breast cancer patients undergoing conservative surgery. Ipsilateral breast tumour recurrence dynamics provides clues for tumour biology within the residual breast
- PMID: 21118508
- PMCID: PMC3002930
- DOI: 10.1186/1471-2407-10-656
Recurrence and mortality according to estrogen receptor status for breast cancer patients undergoing conservative surgery. Ipsilateral breast tumour recurrence dynamics provides clues for tumour biology within the residual breast
Abstract
Background: The study was designed to determine how tumour hormone receptor status affects the subsequent pattern over time (dynamics) of breast cancer recurrence and death following conservative primary breast cancer resection.
Methods: Time span from primary resection until both first recurrence and death were considered among 2825 patients undergoing conservative surgery with or without breast radiotherapy. The hazard rates for ipsilateral breast tumour recurrence (IBTR), distant metastasis (DM) and mortality throughout 10 years of follow-up were assessed.
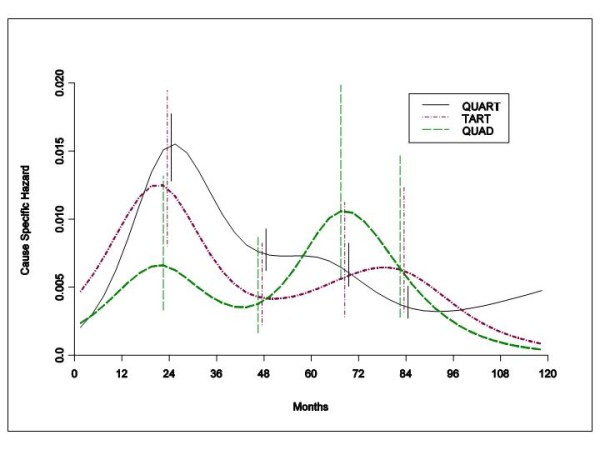
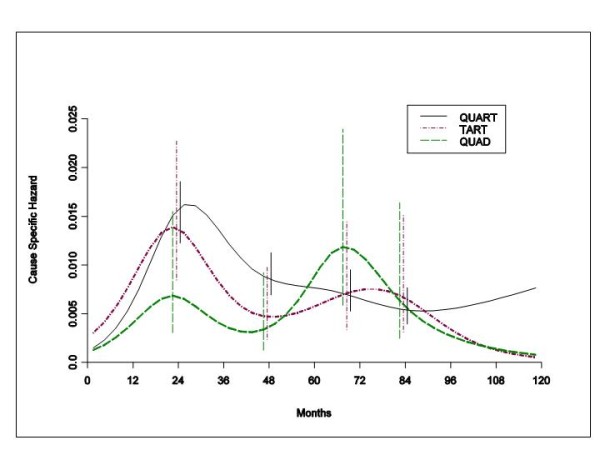
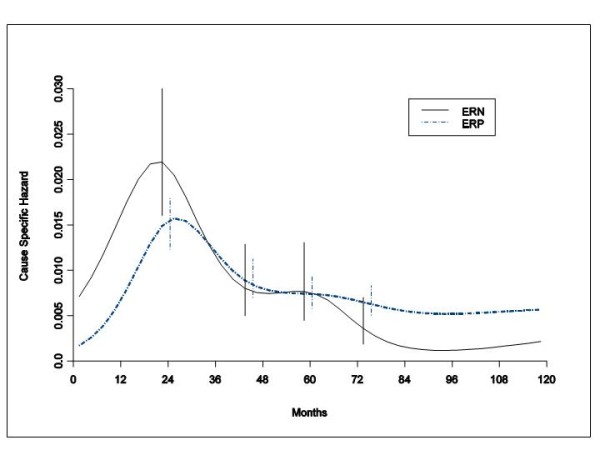
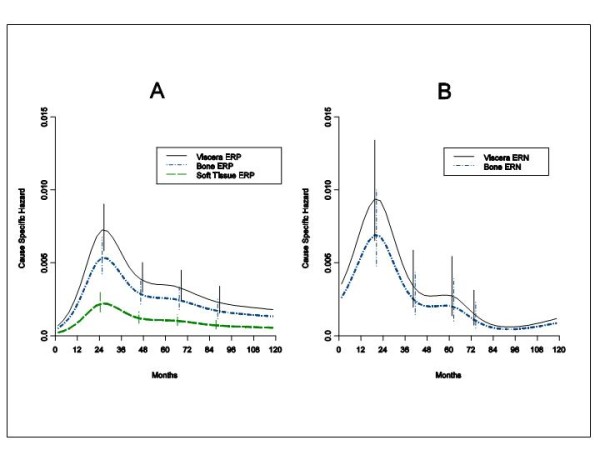
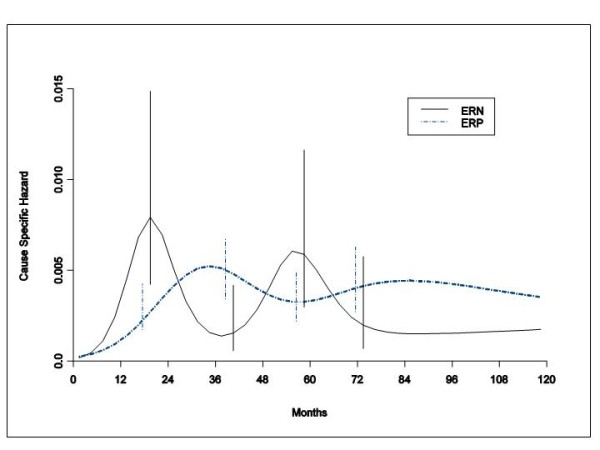
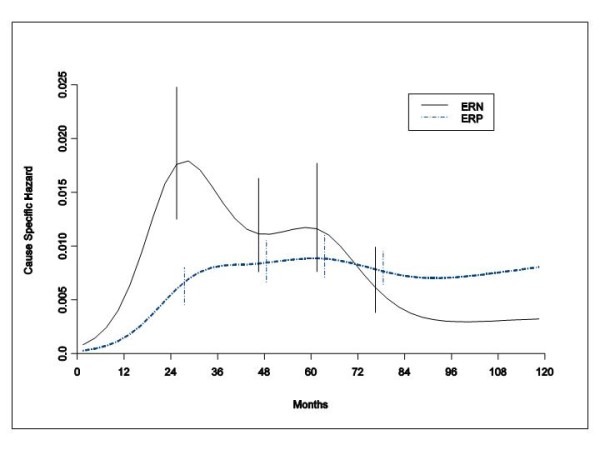
Results: DM dynamics displays the same bimodal pattern (first early peak at about 24 months, second late peak at the sixth-seventh year) for both estrogen receptor (ER) positive (P) and negative (N) tumours and for all local treatments and metastatic sites. The hazard rates for IBTR maintain the bimodal pattern for ERP and ERN tumours; however, each IBTR recurrence peak for ERP tumours is delayed in comparison to the corresponding timing of recurrence peaks for ERN tumours. Mortality dynamics is markedly different for ERP and ERN tumours with more early deaths among patients with ERN than among patients with ERP primary tumours.
Conclusion: DM dynamics is not influenced by the extent of conservative primary tumour resection and is similar for both ER phenotypes across different metastatic sites, suggesting similar mechanisms for tumour development at distant sites despite apparently different microenvironments. The IBTR risk peak delay observed in ERP tumours is an exception to the common recurrence risk rhythm. This suggests that the microenvironment within the residual breast tissue may enforce more stringent constraints upon ERP breast tumour cell growth than other tissues, prolonging the latency of IBTR. This local environment is, however, apparently less constraining to ERN cells, as IBTR dynamics is similar to the corresponding recurrence dynamics among other distant tissues.
Figures
References
-
- Demicheli R, Ardoino I, Biganzoli E, Boracchi P, Coradini D, Greco M, Moliterni A, Zambetti M, Valagussa P, Gukas ID, Bonadonna G. Recurrence and mortality for breast cancer patients undergoing mastectomy according to Estrogen Receptor status: different mortality pattern but comparable recurrence dynamics. Cancer Sci. 2010;101:826–830. doi: 10.1111/j.1349-7006.2009.01472.x. - DOI - PMC - PubMed
