

PD-L1 blockade improves survival in experimental sepsis by inhibiting lymphocyte apoptosis and reversing monocyte dysfunction
- PMID: 21118528
- PMCID: PMC3220038
- DOI: 10.1186/cc9354
PD-L1 blockade improves survival in experimental sepsis by inhibiting lymphocyte apoptosis and reversing monocyte dysfunction
Abstract
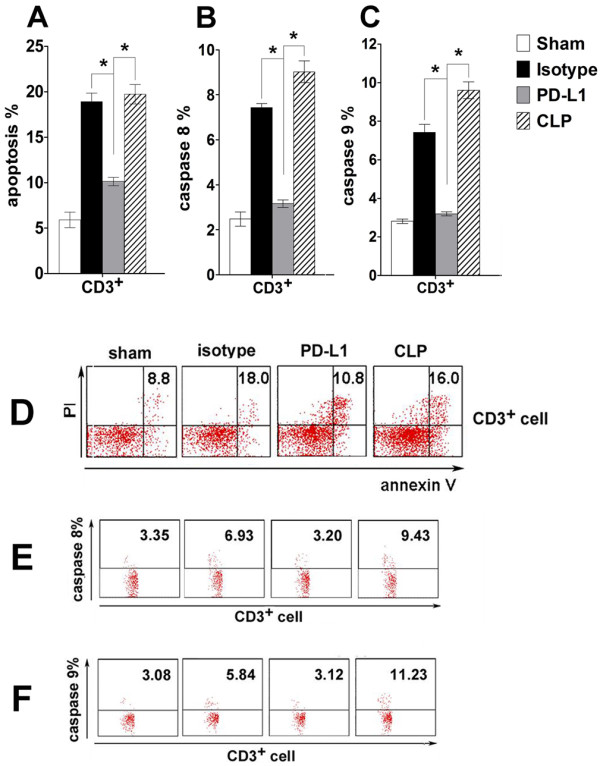
Introduction: Lymphocyte apoptosis and monocyte dysfunction play a pivotal role in sepsis-induced immunosuppression. Programmed death-1 (PD1) and its ligand programmed death ligand-1 (PD-L1) exert inhibitory function by regulating the balance among T cell activation, tolerance, and immunopathology. PD-1 deficiency or blockade has been shown to improve survival in murine sepsis. However, PD-L1 and PD-1 differ in their expression patterns and the role of PD-L1 in sepsis-induced immunosuppression is still unknown.
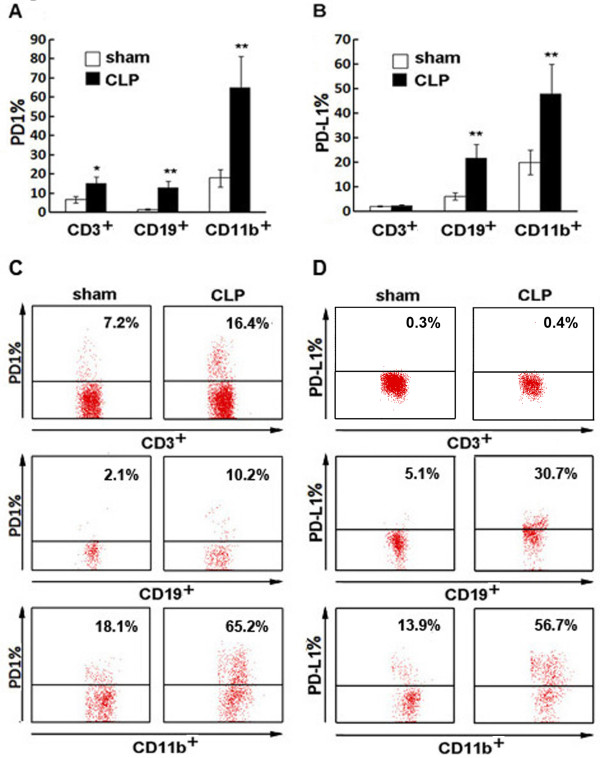
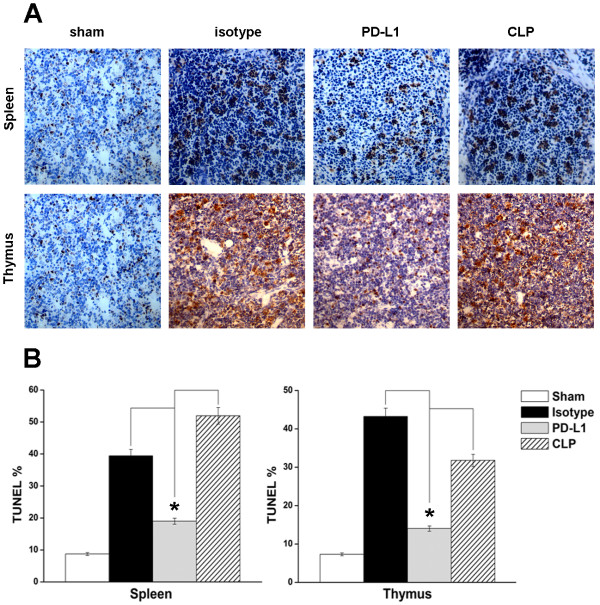
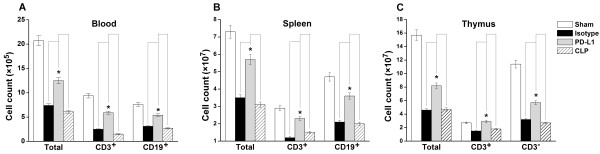
Methods: Sepsis was induced in adult C57BL/6 male mice via cecal ligation and puncture (CLP). The expression of PD-1 and PD-L1 expression on peripheral T cells, B cells and monocytes were measured 24 hours after CLP or sham surgery. Additionally, the effects of anti-PD-L1 antibody on lymphocyte number, apoptosis of spleen and thymus, activities of caspase-8 and caspase-9, cytokine production, bacterial clearance, and survival were determined.
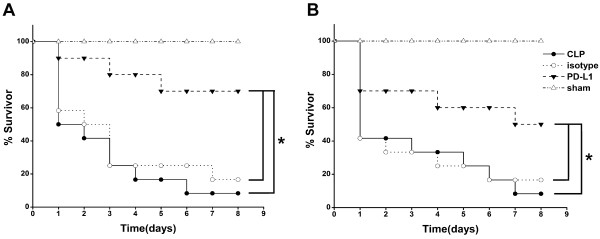
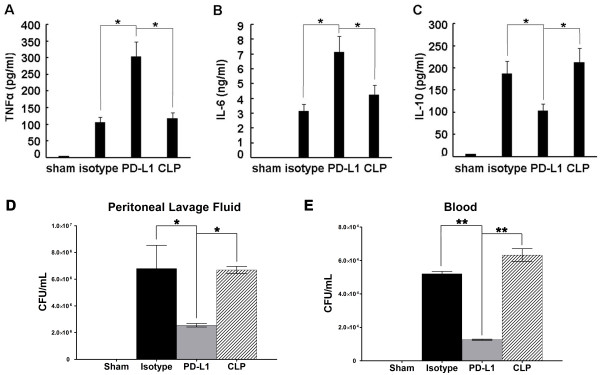
Results: Expression of PD-1 on T cells, B cells and monocytes and PD-L1 on B cells and monocytes were up-regulated in septic animals compared to sham-operated controls. PD-L1 blockade significantly improved survival of CLP mice. Anti-PD-L1 antibody administration prevented sepsis-induced depletion of lymphocytes, increased tumor necrosis factor (TNF)-α and interleukin (IL)-6 production, decreased IL-10 production, and enhanced bacterial clearance.
Conclusions: PD-L1 blockade exerts a protective effect on sepsis at least partly by inhibiting lymphocyte apoptosis and reversing monocyte dysfunction. Anti-PD-L1 antibody administration may be a promising therapeutic strategy for sepsis-induced immunosuppression.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
