

Automated haematology analysis to diagnose malaria
- PMID: 21118557
- PMCID: PMC3013084
- DOI: 10.1186/1475-2875-9-346
Automated haematology analysis to diagnose malaria
Abstract
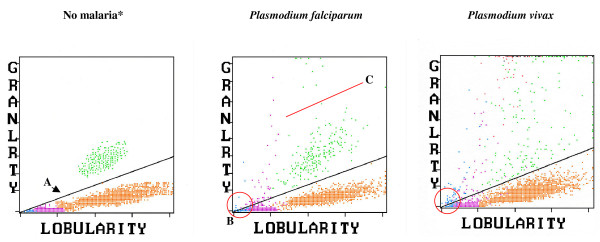
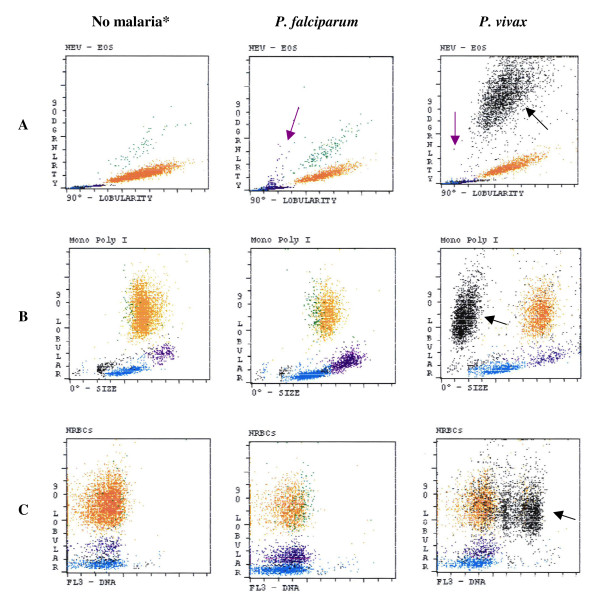
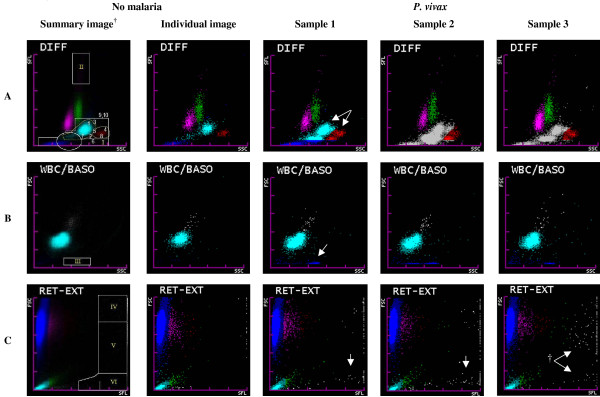
For more than a decade, flow cytometry-based automated haematology analysers have been studied for malaria diagnosis. Although current haematology analysers are not specifically designed to detect malaria-related abnormalities, most studies have found sensitivities that comply with WHO malaria-diagnostic guidelines, i.e. ≥ 95% in samples with > 100 parasites/μl. Establishing a correct and early malaria diagnosis is a prerequisite for an adequate treatment and to minimizing adverse outcomes. Expert light microscopy remains the 'gold standard' for malaria diagnosis in most clinical settings. However, it requires an explicit request from clinicians and has variable accuracy. Malaria diagnosis with flow cytometry-based haematology analysers could become an important adjuvant diagnostic tool in the routine laboratory work-up of febrile patients in or returning from malaria-endemic regions. Haematology analysers so far studied for malaria diagnosis are the Cell-Dyn®, Coulter® GEN·S and LH 750, and the Sysmex XE-2100® analysers. For Cell-Dyn analysers, abnormal depolarization events mainly in the lobularity/granularity and other scatter-plots, and various reticulocyte abnormalities have shown overall sensitivities and specificities of 49% to 97% and 61% to 100%, respectively. For the Coulter analysers, a 'malaria factor' using the monocyte and lymphocyte size standard deviations obtained by impedance detection has shown overall sensitivities and specificities of 82% to 98% and 72% to 94%, respectively. For the XE-2100, abnormal patterns in the DIFF, WBC/BASO, and RET-EXT scatter-plots, and pseudoeosinophilia and other abnormal haematological variables have been described, and multivariate diagnostic models have been designed with overall sensitivities and specificities of 86% to 97% and 81% to 98%, respectively. The accuracy for malaria diagnosis may vary according to species, parasite load, immunity and clinical context where the method is applied. Future developments in new haematology analysers such as considerably simplified, robust and inexpensive devices for malaria detection fitted with an automatically generated alert could improve the detection capacity of these instruments and potentially expand their clinical utility in malaria diagnosis.
Figures
References
-
- Giemsa G. Eine Vereinfachung und Vervollkommnung meiner Methylenblau-Eosin-Färbemethode zur Erzielung der Romanowsky-Nocht'schen Chromatinfärbung. Centralblatt für Bakteriologie. 1904;32:307–313.
-
- Wongsrichanalai C, Barcus MJ, Muth S, Sutamihardja A, Wernsdorfer WH. A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT) Am J Trop Med Hyg. 2007;77:119–127. - PubMed
-
- WHO. New perspectives. Malaria Diagnosis. Report of a Joint WHO/USAID Informal Consultation 25-27 October 1999. Geneva: World Health Organization; 2000.
-
- Gautam AS, Sharma RC, Bhatt RM, Gupta DK. Microscopic diagnosis of malaria in Kheda district of Gujarat. Indian J Malariol. 1992;29:83–87. - PubMed
-
- Durrhelm DN, Becker PJ, Billinghurst K, Brink A. Diagnostic disagreement--the lessons learnt from malaria diagnosis in Mpumalanga. S Afr Med J. 1997;87:609–611. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
