

Explaining variation in referral from primary to secondary care: cohort study
- PMID: 21118873
- PMCID: PMC2995017
- DOI: 10.1136/bmj.c6267
Explaining variation in referral from primary to secondary care: cohort study
Abstract
Objectives: To determine the extent to which referral for defined symptoms from primary care varies by age, sex, and social deprivation and whether any sociodemographic variations in referral differ according to the presence of national referral guidance and the potential of the symptoms to be life threatening.
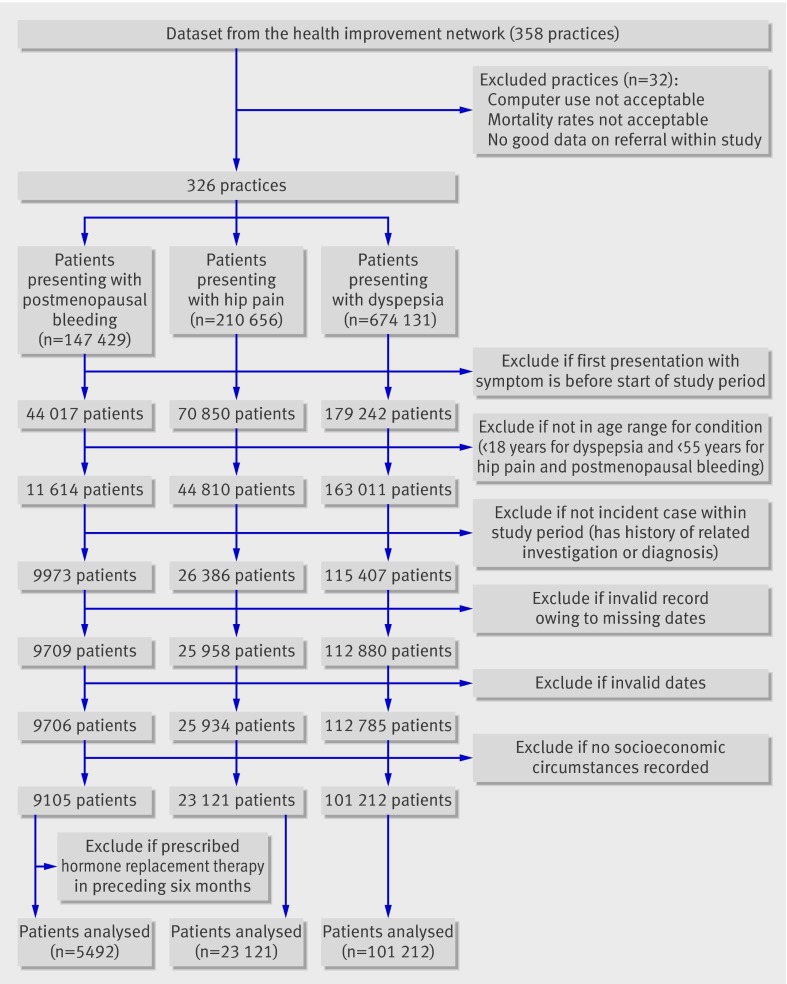
Design: Cohort study using individual patient data from the health improvement network database in primary care.
Setting: United Kingdom.
Participants: 5492 patients with postmenopausal bleeding, 23 121 with hip pain, and 101 212 with dyspepsia from 326 general practices, 2001-7.
Main outcome measures: Multivariable associations between odds of immediate referral for postmenopausal bleeding and age and social deprivation; hazard rates of referral for hip pain or dyspepsia and age, sex, and social deprivation. Analyses for dyspepsia were stratified for people aged less than and more than 55 years because referral guidance differs by age.
Results: 61.4% (3374/5492) of patients with postmenopausal bleeding, 17.4% (4019/23 121) with hip pain, and 13.8% (13 944/101 212) with dyspepsia were referred. The likelihood of referral for postmenopausal bleeding declined with increasing age: the adjusted odds ratio for patients aged 85 or more compared with those aged 55-64 was 0.39 (95% confidence interval 0.31 to 0.49). Patients aged 85 or more with hip pain were also less likely to be referred than those aged 55-64 (0.68, 0.57 to 0.81). Women were less likely than men to be referred for hip pain (hazard ratio 0.90, 95% confidence interval 0.84 to 0.96). More deprived patients with hip pain or dyspepsia (if aged <55) were less likely to be referred. Adjusted hazard ratios for those in the most deprived Townsend fifth compared with the least deprived were 0.72 (95% confidence interval 0.62 to 0.82) and 0.76 (0.68 to 0.85), respectively. No socioeconomic gradient was evident in referral for postmenopausal bleeding.
Conclusions: Inequalities in referral associated with socioeconomic circumstances were more likely to occur in the absence of both explicit guidance and potentially life threatening conditions, whereas inequalities with age were evident for all conditions.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Referral from primary to secondary care.BMJ. 2010 Nov 30;341:c6175. doi: 10.1136/bmj.c6175. BMJ. 2010. PMID: 21118872 No abstract available.
-
Referrals to secondary care. Referral rates for postmenopausal bleeding are not respectable.BMJ. 2010 Dec 30;341:c7407. doi: 10.1136/bmj.c7407. BMJ. 2010. PMID: 21193507 No abstract available.
-
Referrals to secondary care. NICE "referral advice" recommendations database.BMJ. 2011 Jan 11;342:d129. doi: 10.1136/bmj.d129. BMJ. 2011. PMID: 21224319 No abstract available.
References
-
- Campbell SM, Roland MO. Why do people consult the doctor? Fam Pract 1996;13:75-83. - PubMed
-
- Raine R. Does gender bias exist in the use of specialist health care? J Health Serv Res Policy 2000;5:237-49. - PubMed
-
- Department of Health. National service framework for older people. DH, 2001.
-
- Goddard M, Smith P. Equity of access to health care services: theory and evidence from the UK. Soc Sci Med 2001;53:1149-62. - PubMed
-
- Morris S, Sutton M, Gravelle H. Inequity and inequality in the use of health care in England: an empirical investigation. Centre for Health Economics, University of York, 2003. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical