

Neostigmine for the treatment of acute colonic pseudo-obstruction (ACPO) in pediatric hematologic malignancies
- PMID: 21120165
- PMCID: PMC2983008
- DOI: 10.5045/kjh.2010.45.1.62
Neostigmine for the treatment of acute colonic pseudo-obstruction (ACPO) in pediatric hematologic malignancies
Abstract
Background: Acute colonic pseudo-obstruction (ACPO) refers to dilatation of the colon and decreased bowel motility without evidence of mechanical obstruction. Neostigmine, an acetylcholinesterase inhibitor, has been used in patients in whom supportive therapy failed to resolve ACPO. Here, we report the results of administering neostigmine to treat ACPO in children with hematologic malignancies.
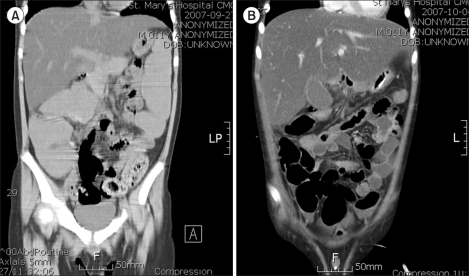
Methods: Between September 2005 and December 2009, 10 patients (8 male and 2 female) were diagnosed with ACPO at the Department of Pediatrics, Catholic University of Korea. Diagnosis of ACPO was based on typical clinical features as well as colonic dilatation found on abdominal CT imaging. Neostigmine was administered subcutaneously at a dosage of 0.01 mg/kg/dose (maximum 0.5 mg) twice daily for a maximum of 5 total doses. ACPO was determined to be responsive to neostigmine if the patient showed both stool passage and improvement of clinical symptoms.
Results: The study group included 8 acute lymphoblastic leukemia patients, 1 patient with malignant lymphoma, and 1 patient with juvenile myelomonocytic leukemia. The median age at ACPO diagnosis was 8.5 years (range, 3-14). Overall, 8 patients (80%) showed therapeutic response to neostigmine at a median of 29 hours after the initial administration (range, 1-70). Two patients (20%) showed side effects of grade 2 or above, but none complained of cardiovascular symptoms that required treatment.
Conclusion: In this study, ACPO was diagnosed most often in late-childhood ALL patients. Subcutaneous neostigmine can be used to effectively treat ACPO diagnosed in children with hematologic malignancies without major cardiovascular complications.
Keywords: Acute colonic pseudo-obstruction; Children; Hematologic malignancies; Neostigmine.
Figures
References
-
- Saunders MD. Acute colonic pseudo-obstruction. Best Pract Res Clin Gastroenterol. 2007;21:671–687. - PubMed
-
- Ponec RJ, Saunders MD, Kimmey MB. Neostigmine for the treatment of acute colonic pseudo-obstruction. N Engl J Med. 1999;341:137–141. - PubMed
-
- van der Spoel JI, Oudemans-van Straaten HM, Stoutenbeek CP, Bosman RJ, Zandstra DF. Neostigmine resolves critical illness-related colonic ileus in intensive care patients with multiple organ failure--a prospective, double-blind, placebo-controlled trial. Intensive Care Med. 2001;27:822–827. - PubMed
-
- McNamara R, Mihalakis MJ. Acute colonic pseudo-obstruction: rapid correction with neostigmine in the emergency department. J Emerg Med. 2008;35:167–170. - PubMed
-
- Rosenberg RF, Caridi JG. Vincristine-induced megacolon. Gastrointest Radiol. 1983;8:71–73. - PubMed
LinkOut - more resources
Full Text Sources
