

Review
doi: 10.1056/NEJMra0910061.
Airway mucus function and dysfunction
Affiliations
- PMID: 21121836
- PMCID: PMC4048736
- DOI: 10.1056/NEJMra0910061
Item in Clipboard
Review
Airway mucus function and dysfunction
N Engl J Med.
.
No abstract available
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
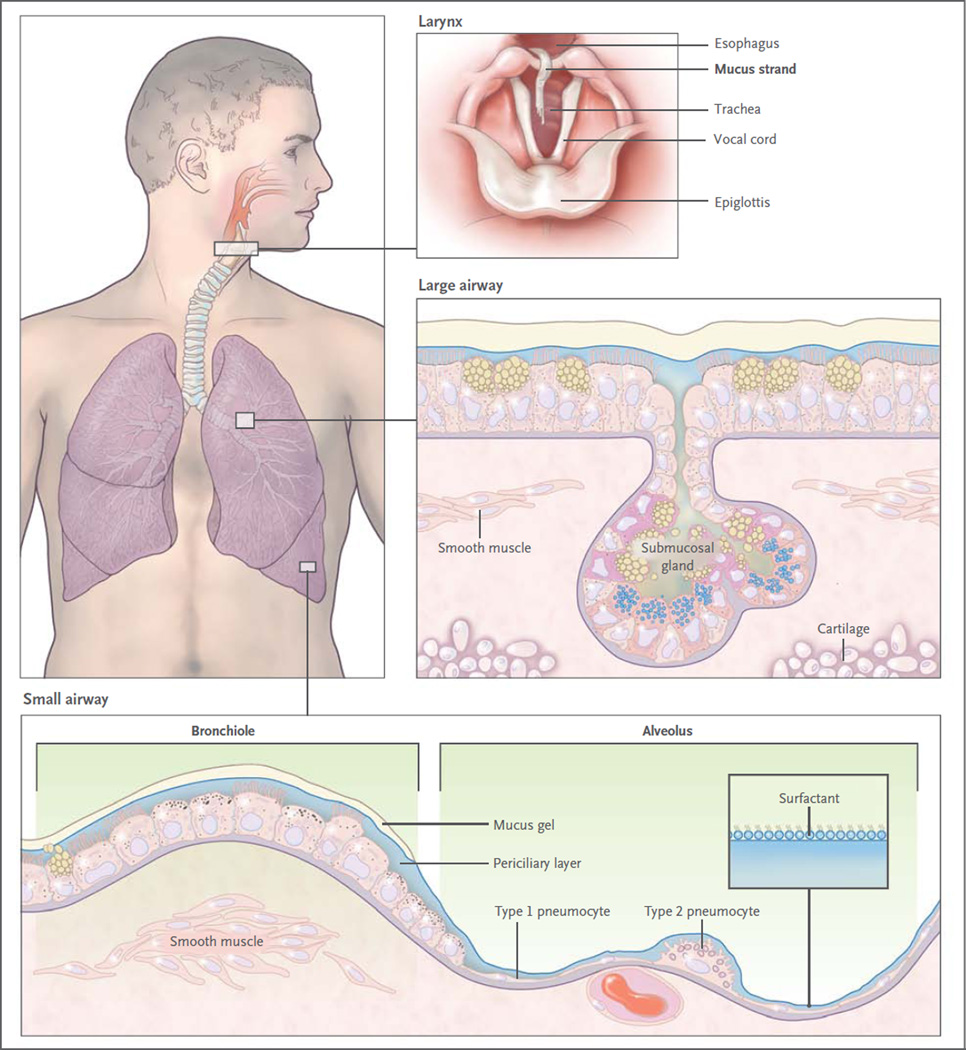
Mucus is continuously swept from distal to proximal airways. In the most distal bronchioles, epithelial cells are cuboidal and do not produce mucin (bottom box), and bronchiolar patency is stabilized by surfactant from adjacent alveoli. In the adjacent small airways, a thin mucus gel layer is produced by columnar secretory (Clara) cells that do not stain for intracellular mucins because they are produced in low amounts and steadily secreted. In the large airways lined by a pseudostratified epithelium, a thick mucus gel layer (up to 50 µm) accumulates from mucus transported from distal airways and additional mucins are produced by surface secretory cells and glands. After mucus ascends the trachea, it is propelled through the vocal cords by ciliary epithelium in the posterior commissure of the larynx. It then enters the pharynx and is swallowed, with approximately 30 ml of airway mucus eliminated by the gastrointestinal tract daily. The vocal cords are covered by squamous epithelium, so they do not participate in ciliary clearance, although they promote cough clearance by closing while expiratory pressure builds and then opening suddenly so airflow is forceful.
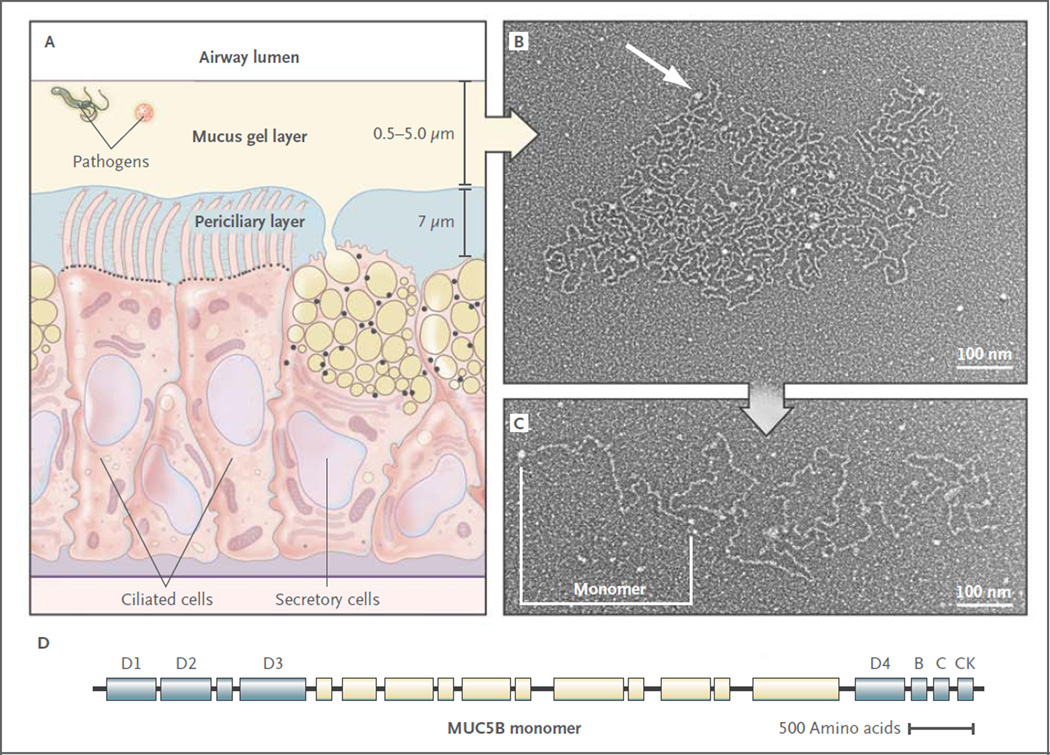
Panel A shows a distal bronchus with a single layer of columnar epithelial cells. The ciliated cells express approximately 200 cilia that are about 7 µm in length. The secretory cells show mixed features of Clara cells (small, black, apical granules containing proteins) and goblet cells (large granules up to 1 µm in diameter containing yellow mucins and black proteins). The mucus gel layer increases in thickness from distal to proximal airways, whereas the periciliary layer is approximately 7 µm deep throughout the conducting airways. Panel B shows an electron micrograph of a partially expanded MUC5B polymer after secretion, intermediate between its condensed form within a secretory granule and its expanded linear structure. Nodes where monomers are bonded appear as white globules (arrow). Panel C shows an electron micrograph of an extended MUC5B polymer. A MUC5B monomer is approximately 450 nm in length, and polymers contain 2 to 20 subunits. Panel D shows the structure of MUC5B. It is organized into an N-terminal region containing von Willebrand factor D1–3 domains involved in N–N polymerization (blue), a central region containing glycosylated mucin domains (pale yellow), and a C-terminal region containing von Willebrand factor D4, B, C, and CK domains involved in C-C polymerization., The structure of MUC5A is similar (not shown). Electron micrographs provided courtesy of Mehmet Kesimer and John K. Sheehan, University of North Carolina.
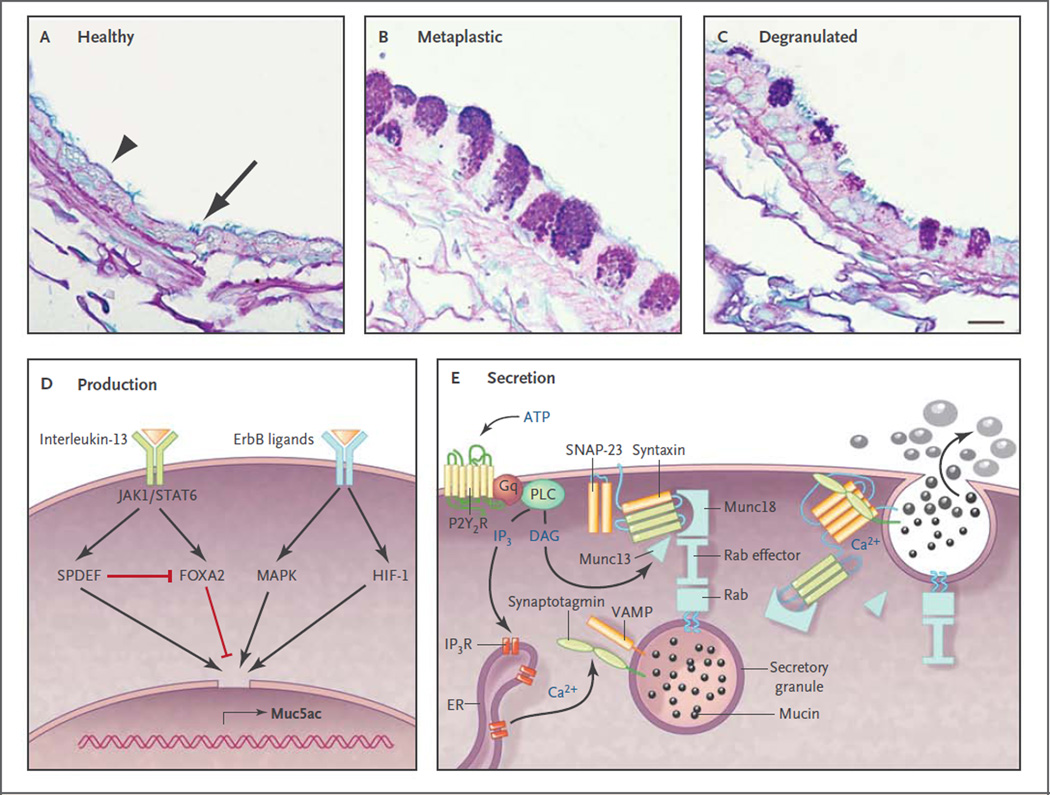
Panels A through C show axial sections through bronchi of mice, which are similar in size and structure to human bronchioles. Panel A shows an airway under healthy conditions, in which polymeric mucin production is low so that the secretory cells (arrowhead) do not show mucin granules when stained with Alcian blue and periodic acid–Schiff reagent. Nonetheless, antibodies indicate that the cells do produce small amounts of Muc5b (not shown), although Muc5ac is undetectable., Ciliated cells are interspersed among the secretory cells (arrow). Panel B shows an airway 2 days after the induction of mucous metaplasia by asthmalike allergic inflammation due to sensitization and challenge with ovalbumin. Mucin-containing granules are visible in the secretory cells as a result of greatly increased Muc5ac and moderately increased Muc5b production.,, Panel C shows a metaplastic airway 10 minutes after stimulation of mucin secretion by an ATP aerosol (scale bar, 10 µm). Panel D shows ligands and transcription factors that are important in Muc5ac expression. Interleukin-13 binds to a receptor that includes the interleukin-4Rα subunit, activating Janus kinase 1 (Jak1), leading to the phosphorylation of Stat6. There is no consensus Stat6 binding site in the MUC5AC and Muc5ac promoter, but Stat6 activation leads to increased expression of SPDEF (SAM pointed domain-containing Ets transcription factor), which up-regulates multiple genes involved in mucous metaplasia, and inhibits expression of Foxa2, which negatively regulates Muc5ac. Several ligands bind ErbB receptors, including epidermal growth factor, transforming growth factor α, amphiregulin, and neuregulin, activating mitogen-activated protein kinases (MAPK)., Hypoxia-inducible factor 1 (HIF-1) also can be activated downstream of ErbB receptors, and there is a conserved HIF-1 binding site in the proximal MUC5AC and Muc5ac promoter, but whether this is the dominant mechanism of up-regulation by ErbB ligands is not known. Not shown are complement C3 and β2-adrenergic–receptor signaling, which amplify Muc5ac production,,– or transcription factors such as Sox2, Notch, E2f4, and Math, which primarily regulate development. Panel E shows the molecular mechanism of mucin exocytosis. A mucin-containing secretory granule is docked to the plasma membrane by the interaction of a granule-bound Rab protein with an effector protein that acts as a tether to Munc18, which binds the closed conformation of Syntaxin anchored to the plasma membrane. Secretion is triggered when ATP binds to P2Y2 purinergic receptors (P2Y2R) coupled to Gq, activating phospholipase C (PLC), which generates the second messengers diacylglycerol (DAG) and inositol triphosphate (IP3). DAG activates Munc13 to open Syntaxin so it can form a four-helix SNARE (soluble N-ethylmaleimide–sensitive factor attachment protein receptor) complex with SNAP-23 (synaptosomal-associated protein 23) and VAMP (vesicle-associated membrane protein), drawing together the granule and plasma membranes. IP3 induces the release of calcium from IP3 receptors (IP3R) in the endoplasmic reticulum (ER), activating Synaptotagmin to induce final coiling of the SNARE complex, which results in fusion of the membranes and release of the mucins. The photomicrographs are courtesy of Dr. Michael J. Tuvim.
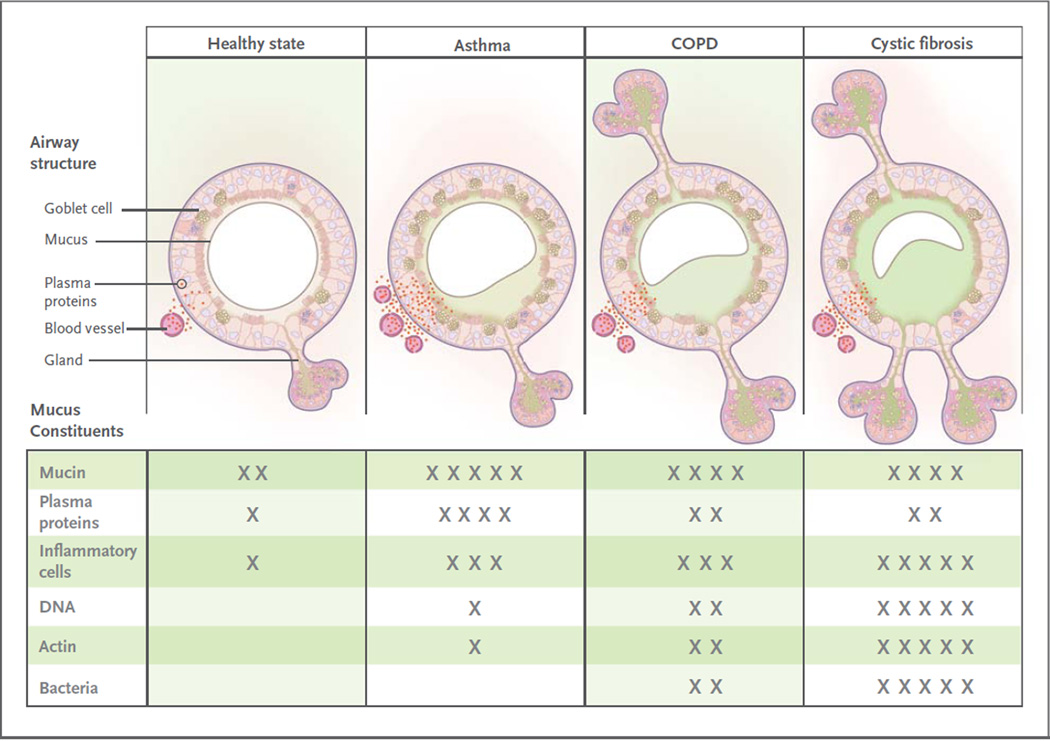
The top panels show the contribution of mucosal disease to abnormal mucus. In asthma, airway remodeling is characterized by increases in epithelial mucin stores because of surface epithelial mucous metaplasia with modest hyperplasia and increased numbers of subepithelial bronchial microvessels that become leaky during inflammation. Changes in submucosal glands are not prominent except in severe disease. In chronic obstructive pulmonary disease (COPD), increased mucin stores occur because of surface epithelial mucous metaplasia and some hyperplasia, together with increases in the volume and number of the submucosal glands. Bronchial microvessel remodeling is not as prominent as in asthma. In cystic fibrosis, epithelial mucin stores are similar to normal levels (possibly because of increased secretion), but submucosal glands are very prominent. Bronchial microvessel remodeling is not as prominent as in asthma. Not shown in the top panels are the increased numbers of inflammatory cells in the airway wall and lumen, which occur in all airway diseases. Products of inflammatory cell death include DNA and actin polymers, which are important constituents of pathologic mucus. The bottom panels list some of the constituents of mucus in health and in airway disease. The degree of cellular inflammation and biochemical constituents of mucus differ among airway diseases. The data for asthma reflect changes that occur in acute severe asthma. The number of Xs indicates the relative abundance of the constituents in each disease state.
Comment in
-
Airway mucus function and dysfunction.N Engl J Med. 2011 Mar 10;364(10):978; author reply 978. doi: 10.1056/NEJMc1014719. N Engl J Med. 2011. PMID: 21388326 No abstract available.
References
-
- Thornton DJ, Sheehan JK. From mucins to mucus: toward a more coherent understanding of this essential barrier. Proc Am Thorac Soc. 2004;1:54–61. - PubMed
-
- Thornton DJ, Rousseau K, McGuckin MA. Structure and function of the polymeric mucins in airways mucus. Annu Rev Physiol. 2008;70:459–486. - PubMed
-
- Rose MC, Voynow JA. Respiratory tract mucin genes and mucin glycoproteins in health and disease. Physiol Rev. 2006;86:245–278. - PubMed
-
- Cone RA. Barrier properties of mucus. Adv Drug Deliv Rev. 2009;61:75–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical