

Renal replacement therapy is an independent risk factor for mortality in critically ill patients with acute kidney injury
- PMID: 21122146
- PMCID: PMC3219996
- DOI: 10.1186/cc9355
Renal replacement therapy is an independent risk factor for mortality in critically ill patients with acute kidney injury
Abstract
Introduction: Outcome studies in patients with acute kidney injury (AKI) have focused on differences between modalities of renal replacement therapy (RRT). The outcome of conservative treatment, however, has never been compared with RRT.
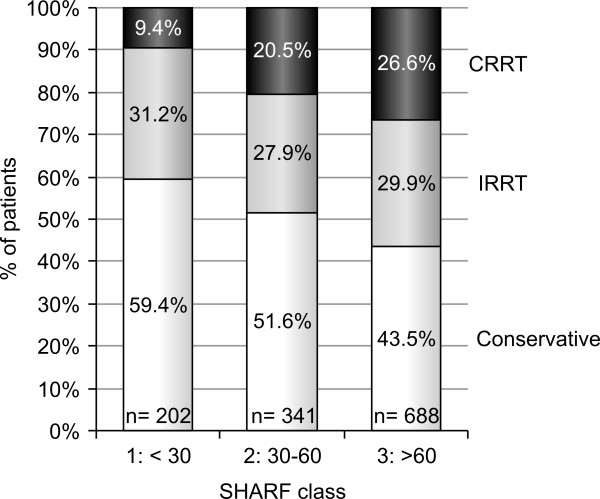
Methods: Nine Belgian intensive care units (ICUs) included all adult patients consecutively admitted with serum creatinine >2 mg/dl. Included treatment options were conservative treatment and intermittent or continuous RRT. Disease severity was determined using the Stuivenberg Hospital Acute Renal Failure (SHARF) score. Outcome parameters studied were mortality, hospital length of stay and renal recovery at hospital discharge.
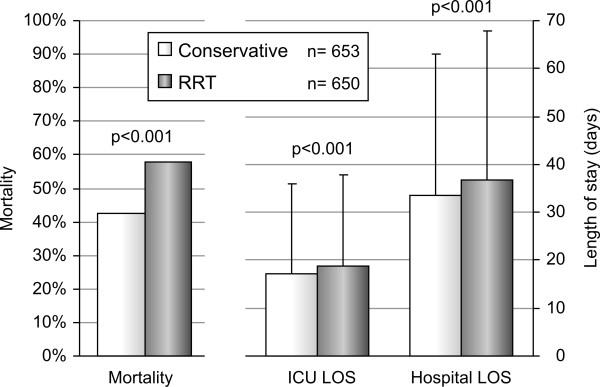
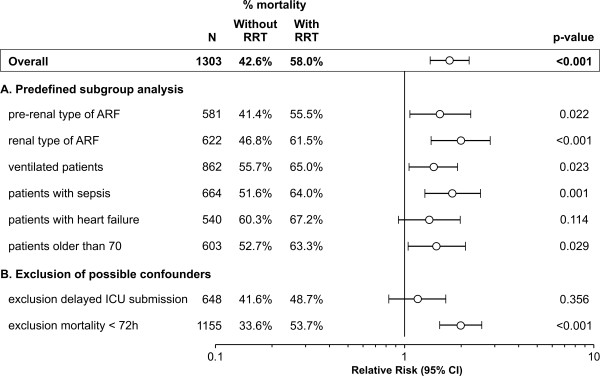
Results: Out of 1,303 included patients, 650 required RRT (58% intermittent, 42% continuous RRT). Overall results showed a higher mortality (43% versus 58%) as well as a longer ICU and hospital stay in RRT patients compared to conservative treatment. Using the SHARF score for adjustment of disease severity, an increased risk of death for RRT compared to conservative treatment of RR = 1.75 (95% CI: 1.4 to 2.3) was found. Additional correction for other severity parameters (Acute Physiology And Chronic Health Evaluation II (APACHE II), Sequential Organ Failure Assessment (SOFA)), age, type of AKI and clinical conditions confirmed the higher mortality in the RRT group.
Conclusions: The SHARF study showed that the higher mortality expected in AKI patients receiving RRT versus conservative treatment can not only be explained by a higher disease severity in the RRT group, even after multiple corrections. A more critical approach to the need for RRT in AKI patients seems to be warranted.
Figures
Comment in
-
Too early initiation of renal replacement therapy may be harmful.Crit Care. 2011;15(1):112. doi: 10.1186/cc9405. Epub 2011 Jan 26. Crit Care. 2011. PMID: 21345253 Free PMC article.
-
Does renal replacement therapy increase mortality in the ICU?Crit Care. 2011;15(2):415; author reply 415. doi: 10.1186/cc10071. Epub 2011 Mar 24. Crit Care. 2011. PMID: 21457492 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
