

Effects of caesarean section on maternal health in low risk nulliparous women: a prospective matched cohort study in Shanghai, China
- PMID: 21122153
- PMCID: PMC3014869
- DOI: 10.1186/1471-2393-10-78
Effects of caesarean section on maternal health in low risk nulliparous women: a prospective matched cohort study in Shanghai, China
Abstract
Background: Rates of caesarean section are progressively increasing in many parts of the world. As a result of psychosocial factors there has been an increasing tendency for pregnant women without justifiable medical indications for caesarean section to ask for this procedure in China. A critical examination of this issue in relation to maternal outcomes is important. At present there are no clinical trials to help assess the risks and benefits of caesarean section in low risk women. To fill the gap left by trials, this indication-matched cohort study was carried out to examine prospectively the outcomes of caesarean section on women with no absolute obstetric indication compared with similar women who had vaginal delivery.
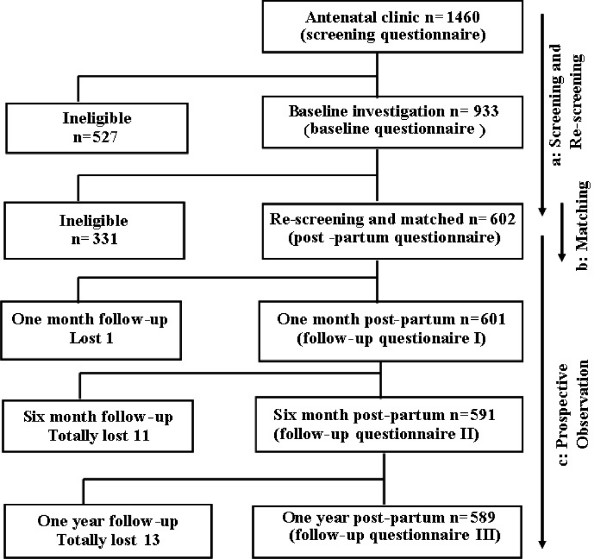
Methods: An indication-matched cohort study was undertaken to compare maternal outcomes following caesarean section with those undergoing vaginal delivery, in which the two groups were matched for non-absolute indications. 301 nulliparous women with caesarean section were matched successfully with 301 women who delivered vaginally in the Maternal and Children's Hospitals (MCHs) in Shanghai, China. Logistic regression model or binomial regression model was used to estimate the relative risk (RR) directly. Adjusted RRs were calculated adjusting for propensity score and medical indications.
Results: The incidence of total complications was 2.2 times higher in the caesarean section group during hospitalization post-partum, compared with the vaginal delivery group (RR = 2.2; 95% CI: 1.1-4.4). The risk of haemorrhage from the start of labour until 2 hours post-partum was significantly higher in the caesarean group (RR = 5.6; 95% CI: 1.2-26.9). The risk of chronic abdominal pain was significantly higher for the caesarean section group (RR = 3.6; 95% CI: 1.2-10.9) than for the vaginal delivery group within 12 months post-partum. The two groups had similar incidences of anaemia and complicating infections such as wound complications or urinary tract infection.
Conclusions: In nulliparous women who were at low risk, caesarean section was associated with a higher rate of post-partum morbidity. Those requesting the surgical procedure with no conventional medical indication, should be advised of the potential risks.
Figures

Similar articles
-
Outcomes of elective labour induction and elective caesarean section in low-risk pregnancies between 37 and 41 weeks' gestation.J Obstet Gynaecol Can. 2009 Dec;31(12):1124-30. doi: 10.1016/s1701-2163(16)34372-9. J Obstet Gynaecol Can. 2009. PMID: 20085677
-
Maternal and infant outcome after caesarean section without recorded medical indication: findings from a Swedish case-control study.BJOG. 2013 Mar;120(4):479-86; discussion 486. doi: 10.1111/1471-0528.12129. Epub 2013 Jan 15. BJOG. 2013. PMID: 23316937
-
Elective cesarean section or not? Maternal age and risk of adverse outcomes at term: a population-based registry study of low-risk primiparous women.BMC Pregnancy Childbirth. 2016 Aug 17;16:230. doi: 10.1186/s12884-016-1028-3. BMC Pregnancy Childbirth. 2016. PMID: 27535233 Free PMC article.
-
Mechanical dilatation of the cervix during elective caeserean section before the onset of labour for reducing postoperative morbidity.Cochrane Database Syst Rev. 2018 Aug 10;8(8):CD008019. doi: 10.1002/14651858.CD008019.pub3. Cochrane Database Syst Rev. 2018. PMID: 30096215 Free PMC article.
-
Different classes of antibiotics given to women routinely for preventing infection at caesarean section.Cochrane Database Syst Rev. 2021 Mar 4;3(3):CD008726. doi: 10.1002/14651858.CD008726.pub3. Cochrane Database Syst Rev. 2021. PMID: 33661539 Free PMC article.
Cited by
-
Combined laparoscopy and hysteroscopy vs. uterine curettage in the uterine artery embolization-based management of cesarean scar pregnancy: a cohort study.Int J Clin Exp Med. 2014 Sep 15;7(9):2793-803. eCollection 2014. Int J Clin Exp Med. 2014. PMID: 25356141 Free PMC article.
-
Implementation and evaluation of nonclinical interventions for appropriate use of cesarean section in low- and middle-income countries: protocol for a multisite hybrid effectiveness-implementation type III trial.Implement Sci. 2020 Sep 4;15(1):72. doi: 10.1186/s13012-020-01029-4. Implement Sci. 2020. PMID: 32887669 Free PMC article.
-
Factors influencing attempted and completed suicide in postnatal women: A population-based study in Taiwan.Sci Rep. 2016 May 12;6:25770. doi: 10.1038/srep25770. Sci Rep. 2016. PMID: 27173845 Free PMC article.
-
Preference for institutional delivery and caesarean sections in Bangladesh.J Health Popul Nutr. 2013 Mar;31(1):96-109. doi: 10.3329/jhpn.v31i1.14754. J Health Popul Nutr. 2013. PMID: 23617210 Free PMC article.
-
Socioeconomic inequalities in skilled attendance at birth and caesarean section rates in Myanmar 2015-2016: a cross-sectional study.BMJ Open. 2024 Mar 18;14(3):e076646. doi: 10.1136/bmjopen-2023-076646. BMJ Open. 2024. PMID: 38503412 Free PMC article.
References
-
- Duan T. Present situation and some thoughts of caesarean section. Chinese Journal of Practical Gynecology and Obstetrics. 2008;24:721–723.
-
- World Health Organization. Appropriate technology for birth. Lancet. 1985;2:436–437. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
