

doi: 10.1186/alzrt56.
Use of theragnostic markers to select drugs for phase II/III trials for Alzheimer disease
Affiliations
- PMID: 21122172
- PMCID: PMC3031878
- DOI: 10.1186/alzrt56
Item in Clipboard
Use of theragnostic markers to select drugs for phase II/III trials for Alzheimer disease
Alzheimers Res Ther.
.
Abstract
In a slowly progressive disorder like Alzheimer disease, evaluation of the clinical effect of novel drug candidates requires large numbers of patients and extended treatment periods. Current cell- and animal-based disease models of Alzheimer disease are poor at predicting a positive treatment response in patients. To help bridge the gap between disease models and large and costly clinical trials with high failure rates, biomarkers for the intended biochemical drug effect may be of value. Such biomarkers may be called 'theragnostic'. Here, we review the literature addressing the prospective value of these biomarkers.
Figures
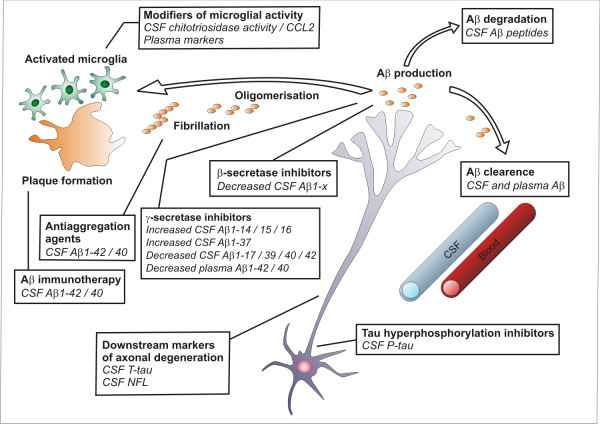
Summary of candidate theragnostic biomarkers that reflect key drug targets in the Alzheimer disease (AD) process. Beta-secretase inhibitors should reduce cerebrospinal fluid (CSF) levels of amyloid beta (Aβ) isoforms starting at the first amino acid in the Aβ sequence (Aβ1-X). Gamma-secretase inhibitors should reduce Aβ1-40 and Aβ1-42 and increase Aβ1-14, Aβ1-15, and Aβ1-16. Both Aβ immunotherapy and anti-aggregation agents might be monitored by CSF levels of Aβ1-40 and Aβ1-42. Therapy-induced Aβ degradation might be monitored by CSF levels of different Aβ peptides, depending on the proteolytic pathway used for degradation. Aβ efflux from the brain to the blood might be monitored by measurement of Aβ in CSF and plasma. Inflammatory markers in plasma and CSF as well as CSF levels of CCL2 and chitotriosidase activity are putative markers of microglial activity and may change in response to treatments that influence microglial activity. Treatment with tau hyperphosphorylation inhibitors might be monitored with CSF phospho-tau (P-tau) levels. Downstream effects on axonal degeneration from disease-modifying treatments could be monitored by using the axonal damage markers CSF total tau (T-tau) and neurofilament light protein (NFL).
Similar articles
-
Biomarkers for the early stages of clinical development in Alzheimer's disease.Therapie. 2010 Jul-Aug;65(4):285-90, 277-283. doi: 10.2515/therapie/2010040. Epub 2010 Sep 21. Therapie. 2010. PMID: 20854749 Review. English, French.
-
Clinical Theragnostic Potential of Diverse miRNA Expressions in Prostate Cancer: A Systematic Review and Meta-Analysis.Cancers (Basel). 2020 May 9;12(5):1199. doi: 10.3390/cancers12051199. Cancers (Basel). 2020. PMID: 32397507 Free PMC article.
-
Evaluation of the performance of novel Aβ isoforms as theragnostic markers in Alzheimer's disease: from the cell to the patient.Neurodegener Dis. 2012;10(1-4):138-40. doi: 10.1159/000334537. Epub 2012 Feb 1. Neurodegener Dis. 2012. PMID: 22302034 Review.
-
Biomarkers in Alzheimer's disease drug development.Nat Med. 2010 Nov;16(11):1218-22. doi: 10.1038/nm.2221. Epub 2010 Sep 21. Nat Med. 2010. PMID: 21052077
-
The discovery and development of proteomic safety biomarkers for the detection of drug-induced liver toxicity.Toxicol Appl Pharmacol. 2010 May 15;245(1):134-42. doi: 10.1016/j.taap.2010.02.011. Epub 2010 Feb 26. Toxicol Appl Pharmacol. 2010. PMID: 20219512 Review.
Cited by
-
Use of biomarkers and imaging to assess pathophysiology, mechanisms of action and target engagement.J Nutr Health Aging. 2013 Jan;17(1):54-63. doi: 10.1007/s12603-013-0003-1. J Nutr Health Aging. 2013. PMID: 23299381
-
NOTCH inhibits osteoblast formation in inflammatory arthritis via noncanonical NF-κB.J Clin Invest. 2014 Jul;124(7):3200-14. doi: 10.1172/JCI68901. Epub 2014 Jun 2. J Clin Invest. 2014. PMID: 24892805 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
