

Severe mood dysregulation, irritability, and the diagnostic boundaries of bipolar disorder in youths
- PMID: 21123313
- PMCID: PMC3396206
- DOI: 10.1176/appi.ajp.2010.10050766
Severe mood dysregulation, irritability, and the diagnostic boundaries of bipolar disorder in youths
Abstract
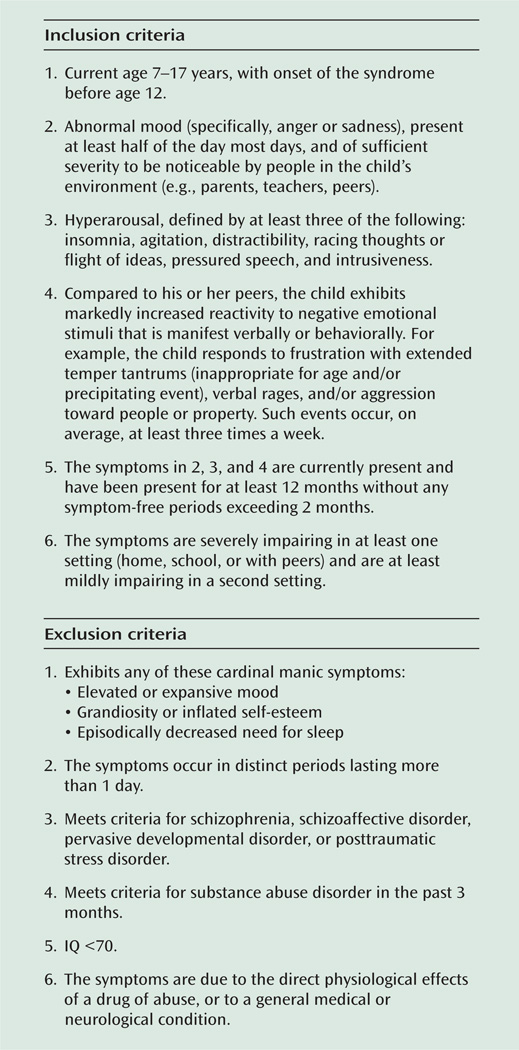
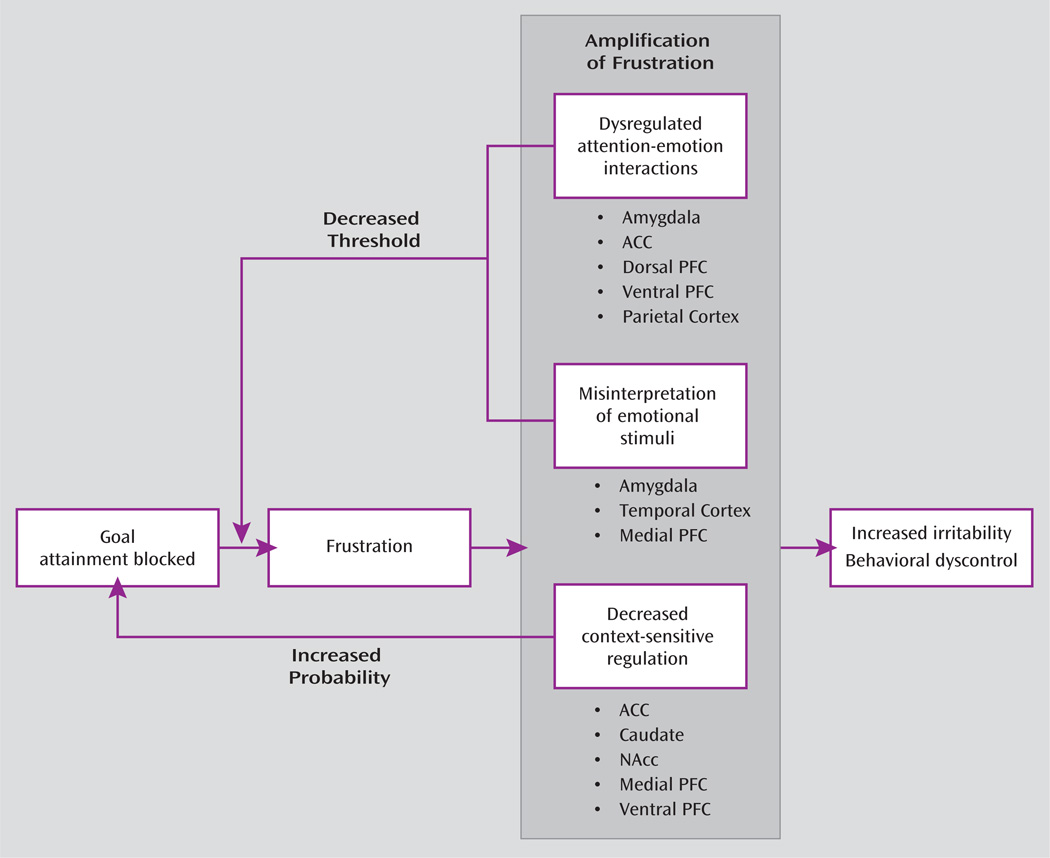
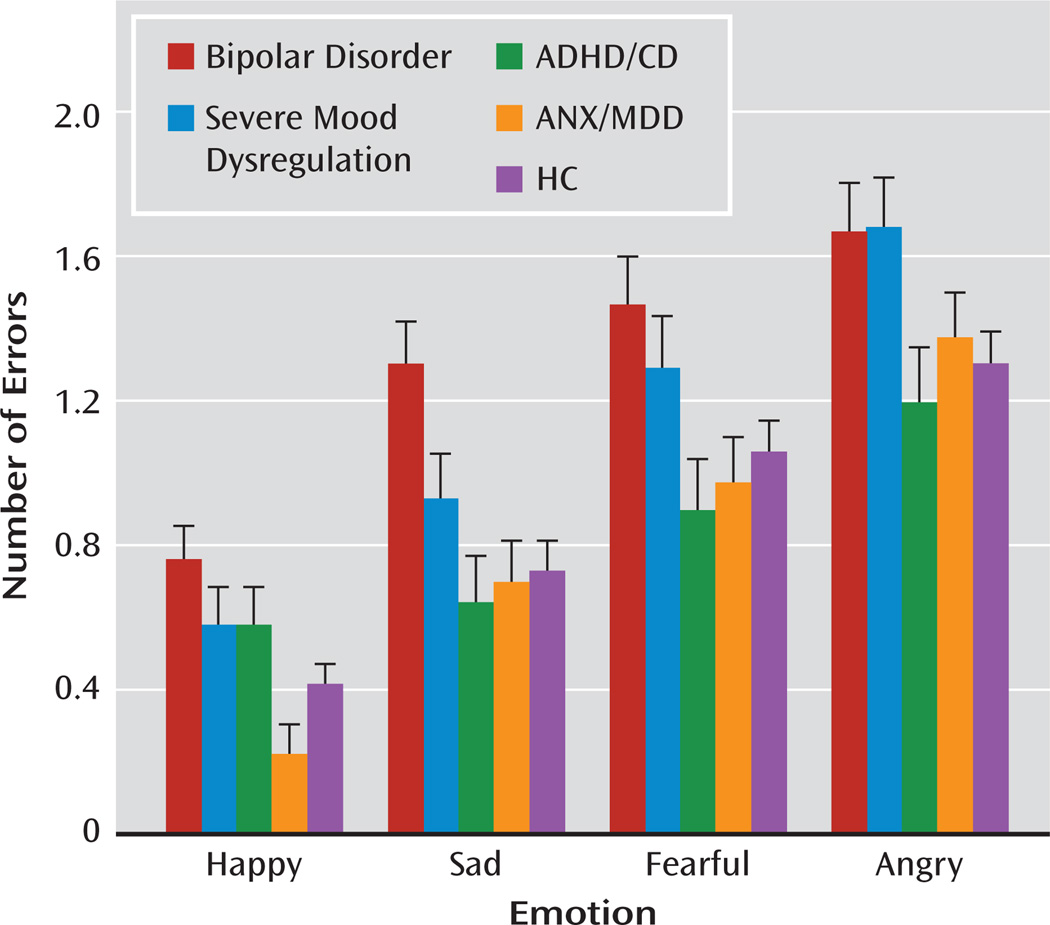
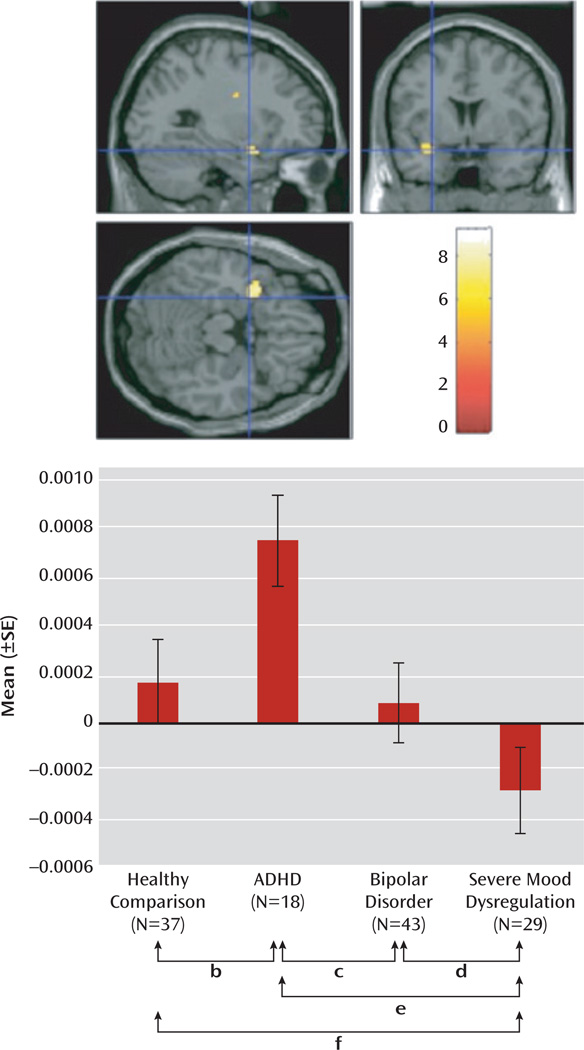
In recent years, increasing numbers of children have been diagnosed with bipolar disorder. In some cases, children with unstable mood clearly meet current diagnostic criteria for bipolar disorder, and in others, the diagnosis is unclear. Severe mood dysregulation is a syndrome defined to capture the symptomatology of children whose diagnostic status with respect to bipolar disorder is uncertain, that is, those who have severe, nonepisodic irritability and the hyperarousal symptoms characteristic of mania but who lack the well-demarcated periods of elevated or irritable mood characteristic of bipolar disorder. Levels of impairment are comparable between youths with bipolar disorder and those with severe mood dysregulation. An emerging literature compares children with severe mood dysregulation and those with bipolar disorder in longitudinal course, family history, and pathophysiology. Longitudinal data in both clinical and community samples indicate that nonepisodic irritability in youths is common and is associated with an elevated risk for anxiety and unipolar depressive disorders, but not bipolar disorder, in adulthood. Data also suggest that youths with severe mood dysregulation have lower familial rates of bipolar disorder than do those with bipolar disorder. While youths in both patient groups have deficits in face emotion labeling and experience more frustration than do normally developing children, the brain mechanisms mediating these pathophysiologic abnormalities appear to differ between the two patient groups. No specific treatment for severe mood dysregulation currently exists, but verification of its identity as a syndrome distinct from bipolar disorder by further research should include treatment trials.
Figures
References
-
- Moreno C, Laje G, Blanco C, Jiang H, Schmidt AB, Olfson M. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry. 2007;64:1032–1039. - PubMed
-
- Biederman J, Klein RG, Pine DS, Klein DF. Resolved: mania is mistaken for ADHD in prepubertal children. J Am Acad Child Adolesc Psychiatry. 1998;37:1091–1099. - PubMed
-
- Biederman J, Faraone SV, Wozniak J, Mick E, Kwon A, Aleardi M. Further evidence of unique developmental phenotypic correlates of pediatric bipolar disorder: findings from a large sample of clinically referred preadolescent children assessed over the last 7 years. J Affect Disord. 2004;82(suppl):S45–S58. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
