

Community based integrated intervention for prevention and management of chronic obstructive pulmonary disease (COPD) in Guangdong, China: cluster randomised controlled trial
- PMID: 21123342
- PMCID: PMC2995286
- DOI: 10.1136/bmj.c6387
Community based integrated intervention for prevention and management of chronic obstructive pulmonary disease (COPD) in Guangdong, China: cluster randomised controlled trial
Abstract
Objective: To evaluate the effects of a community based integrated intervention for early prevention and management of chronic obstructive pulmonary disease (COPD) in China.
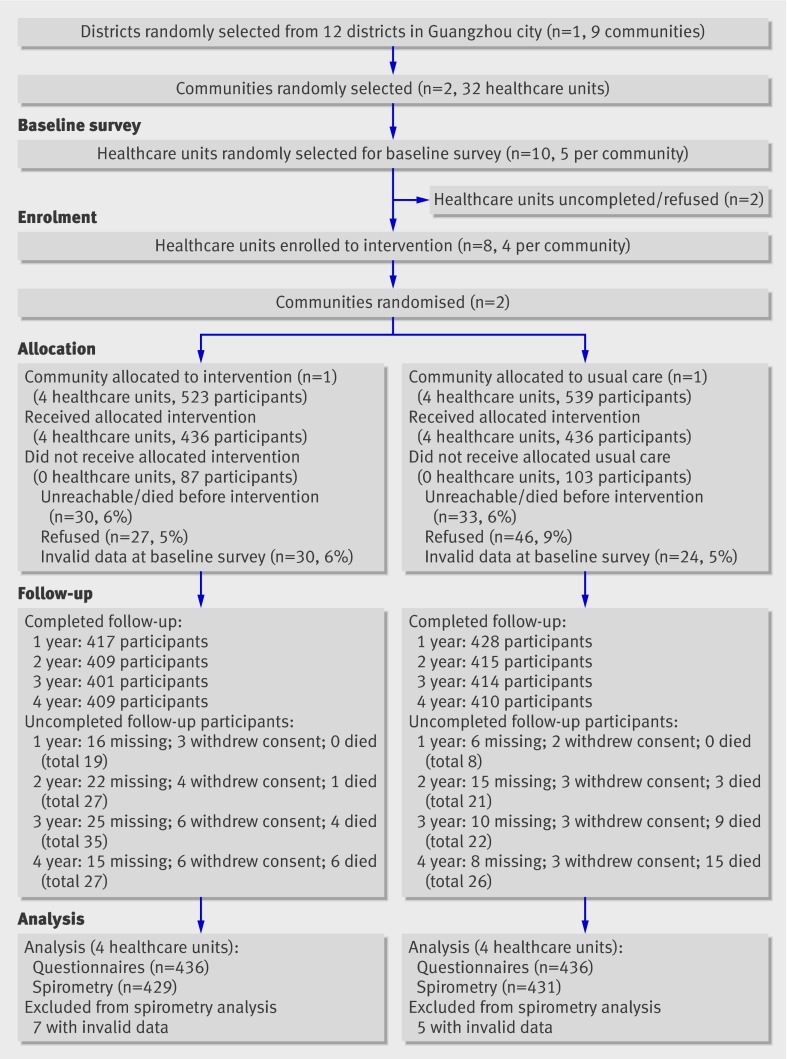
Design: Cluster randomised controlled trial.
Setting: Eight healthcare units in two communities.
Participants: Of 1062 people aged 40-89, 872 (101 with COPD and 771 without COPD) who fulfilled the inclusion and exclusion criteria were allocated to the intervention or the usual care programmes.
Intervention: Participants randomly assigned to integrated intervention (systematic health education, intensive and individualised intervention, treatment, and rehabilitation) or usual care.
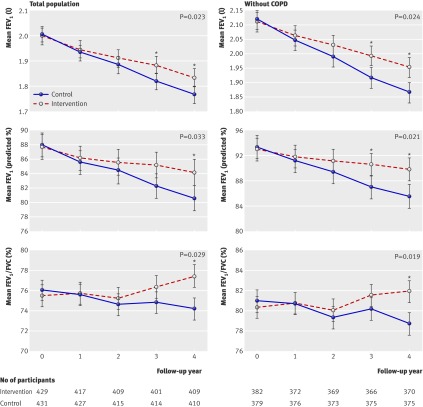
Main outcome measures: Annual rate of decline in forced expiratory rate in one second (FEV(1)) before use of bronchodilator.
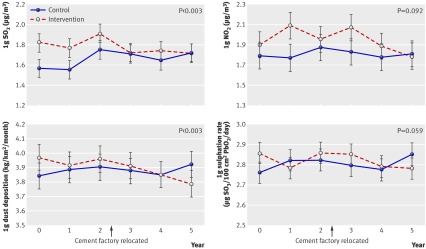
Results: Annual rate of decline in FEV(1) was significantly lower in the intervention community than the control community, with an adjusted difference of 19 ml/year (95% confidence interval 3 to 36) and 0.9% (0.1% to 1.8%) of predicted values (all P<0.05), as well as a lower annual rate of decline in FEV(1)/FVC (forced vital capacity) ratio (adjusted difference 0.6% (0.1% to 1.2%) P=0.029). There were also higher rates of smoking cessation (21% v 8%, P<0.004) and lower cumulative death rates from all causes (1% v 3%, P<0.009) in the intervention community than in the control community during the four year follow-up. Improvements in knowledge of COPD and smoking hazards, outdoor air quality, environmental tobacco smoke, and working conditions were also achieved (all P<0.05). The difference in cumulative incidence rate of COPD (both around 4%) and cumulative death rate from COPD (2% v 11%) did not reach significance between the two communities.
Conclusions: A community based integrated intervention can have a significant impact on the prevention and management of COPD, mainly reflected in the annual rate of decline in FEV(1).
Trial registration: Chinese Clinical Trials Registration (ChiCTR-TRC-00000532).
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Sin DD, Stafinski The impact of chronic obstructive pulmonary disease on work loss in the United States. Am J Respir Crit Care Med 2002;165:704-7. - PubMed
-
- Lopez AD, Murray CC. The global burden of disease, 1990-2020. Nat Med 1998;4:1241-3. - PubMed
-
- Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, et al. International variation in the prevalence of COPD (the burden of obstructive lung disease study): a population-based prevalence study. Lancet 2007;370:741-50. - PubMed
-
- Zhong N, Wang C, Yao W, Chen P, Kang J, Huang S, et al. Prevalence of chronic obstructive pulmonary disease in China—a large population-based spirometry based cross-sectional survey. Am J Respir Crit Care Med 2007;176:753-60. - PubMed
-
- Chan-Yeung M, Aït-Khaled N, White N, Ip MS, Tan WC. The burden and impact of COPD in Asia and Africa. Int J Tuberc Lung Dis 2004;8:2-14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical