

Advances and challenges in malaria vaccine development
- PMID: 21123952
- PMCID: PMC2994342
- DOI: 10.1172/JCI44423
Advances and challenges in malaria vaccine development
Abstract
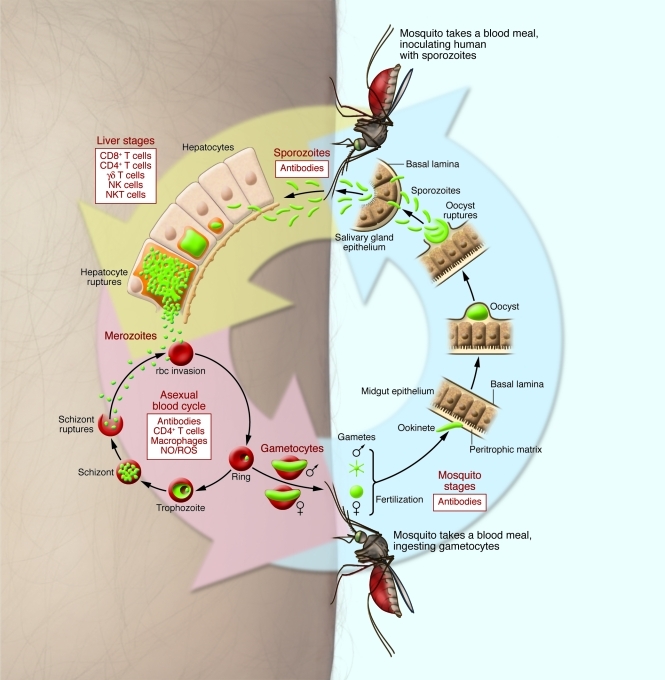
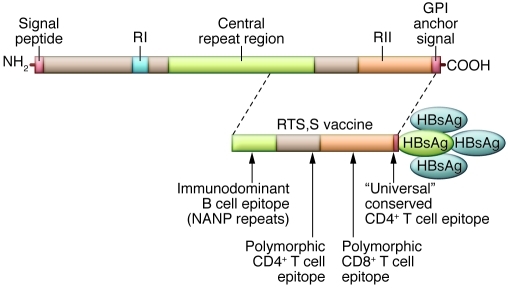
Malaria caused by Plasmodium falciparum remains a major public health threat, especially among children and pregnant women in Africa. An effective malaria vaccine would be a valuable tool to reduce the disease burden and could contribute to elimination of malaria in some regions of the world. Current malaria vaccine candidates are directed against human and mosquito stages of the parasite life cycle, but thus far, relatively few proteins have been studied for potential vaccine development. The most advanced vaccine candidate, RTS,S, conferred partial protection against malaria in phase II clinical trials and is currently being evaluated in a phase III trial in Africa. New vaccine targets need to be identified to improve the chances of developing a highly effective malaria vaccine. A better understanding of the mechanisms of naturally acquired immunity to malaria may lead to insights for vaccine development.
Figures
References
-
- WHO. WHO World Malaria Report 2008. World Health Organization Web Site. http://www.who.int/malaria/publications/atoz/9789241563697/en/index.html . Accessed October 8, 2010.
-
- Johansson EW, Cibulskis R, Steketee RW. Malaria funding and resource utilization: the first decade of roll back malaria. In:Roll Back Malaria Progress & Impact Series . Number 1. Geneva, Switzerland: World Health Organization; 2010.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
