

Cost-effectiveness of antiretroviral regimens in the World Health Organization's treatment guidelines: a South African analysis
- PMID: 21124202
- PMCID: PMC3071983
- DOI: 10.1097/QAD.0b013e328340fdf8
Cost-effectiveness of antiretroviral regimens in the World Health Organization's treatment guidelines: a South African analysis
Abstract
Objective: the World Health Organization (WHO) recently changed its first-line antiretroviral treatment guidelines in resource-limited settings. The cost-effectiveness of the new guidelines is unknown.
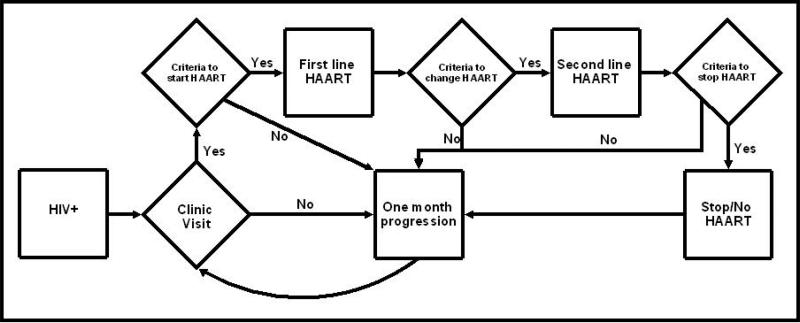
Design: comparative effectiveness and cost-effectiveness analysis using a model of HIV disease progression and treatment.
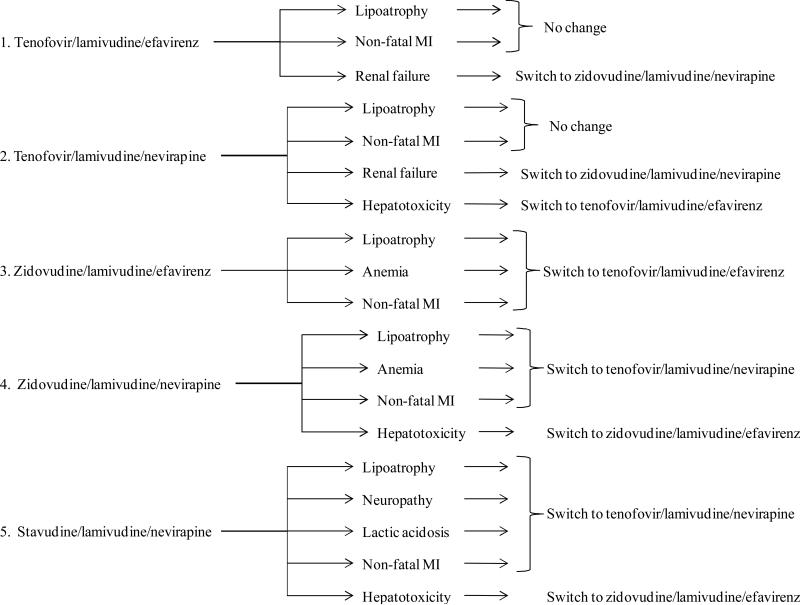
Methods: using a simulation of HIV disease and treatment in South Africa, we compared the life expectancy, quality-adjusted life expectancy, lifetime costs, and cost-effectiveness of five initial regimens. Four are currently recommended by the WHO: tenofovir/lamivudine/efavirenz; tenofovir/lamivudine/nevirapine; zidovudine/lamivudine/efavirenz; and zidovudine/lamivudine/nevirapine. The fifth is the most common regimen in current use: stavudine/lamivudine/nevirapine. Virologic suppression and toxicities determine regimen effectiveness and cost-effectiveness.
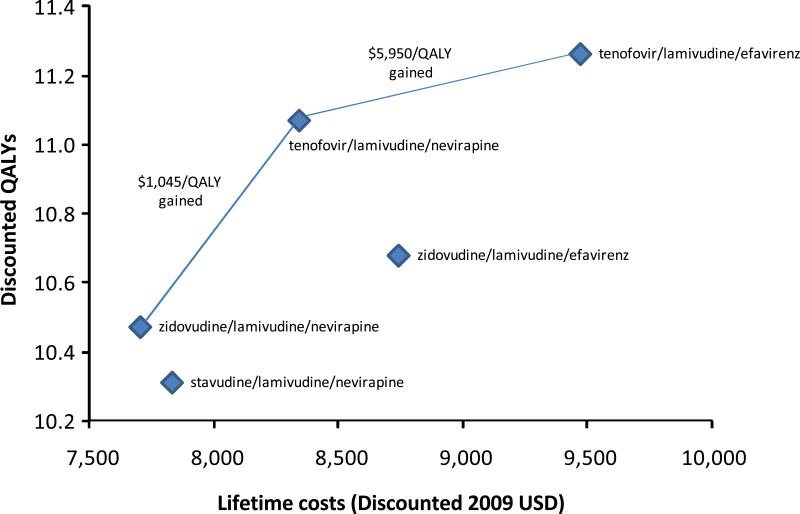
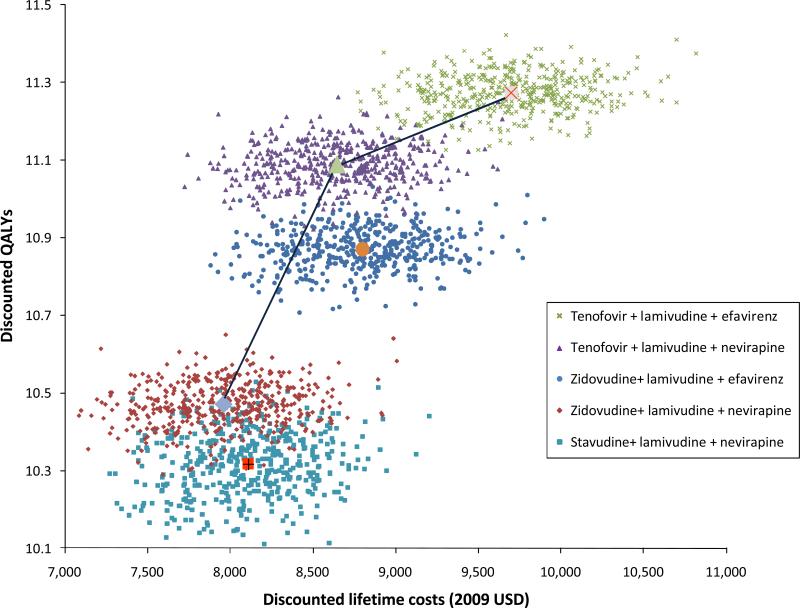
Results: choice of first-line regimen is associated with a difference of nearly 12 months of quality-adjusted life expectancy, from 135.2 months (tenofovir/lamivudine/efavirenz) to 123.7 months (stavudine/lamivudine/nevirapine). Stavudine/lamivudine/nevirapine is more costly and less effective than zidovudine/lamivudine/nevirapine. Initiating treatment with a regimen containing tenofovir/lamivudine/nevirapine is associated with an incremental cost-effectiveness ratio of $1045 per quality-adjusted life year compared with zidovudine/lamivudine/nevirapine. Using tenofovir/lamivudine/efavirenz was associated with the highest survival, fewest opportunistic diseases, lowest rate of regimen substitution, and an incremental cost-effectiveness ratio of $5949 per quality-adjusted life year gained compared with tenofovir/lamivudine/nevirapine. Zidovudine/lamivudine/efavirenz was more costly and less effective than tenofovir/lamivudine/nevirapine. Results were sensitive to the rates of toxicities and the disutility associated with each toxicity.
Conclusion: among the options recommended by WHO, we estimate only three should be considered under normal circumstances. Choice among those depends on available resources and willingness to pay. Stavudine/lamivudine/nevirapine is associated with the poorest quality-adjusted survival and higher costs than zidovudine/lamivudine/nevirapine.
2011 Wolters Kluwer Health | Lippincott Williams & Wilkins.
Figures
References
-
- Rapid Advice: Antiretroviral Therapy for HIV Infection in Adults and Adolescents. World Health Organization; Geneva: Nov, 2009. - PubMed
-
- Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. Jan 25, 2009. 2010. Available from: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
-
- Gazzard B. British HIV Association guidelines for the treatment of HIV-1-infected adults with antiretroviral therapy 2008. HIV medicine. 2008;9(8):563. - PubMed
-
- Hammer SM, et al. Antiretroviral treatment of adult HIV infection: 2008 recommendations of the International AIDS Society-USA panel. Jama. 2008;300(5):555–70. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
