

Different mechanisms for heterogeneity in leprosy susceptibility can explain disease clustering within households
- PMID: 21124916
- PMCID: PMC2988824
- DOI: 10.1371/journal.pone.0014061
Different mechanisms for heterogeneity in leprosy susceptibility can explain disease clustering within households
Abstract
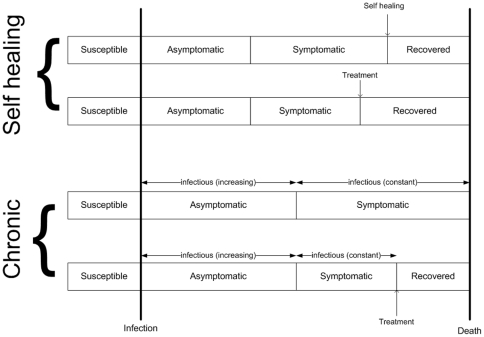
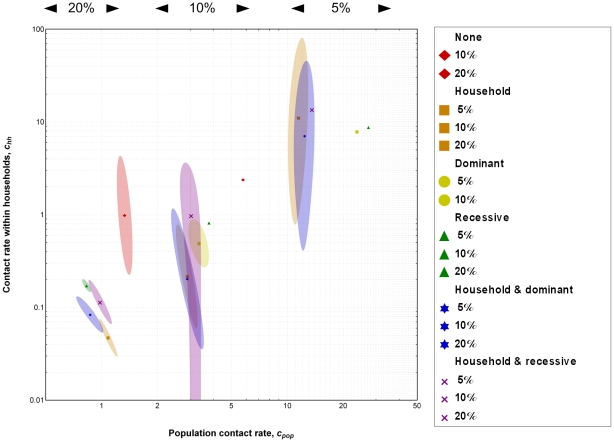
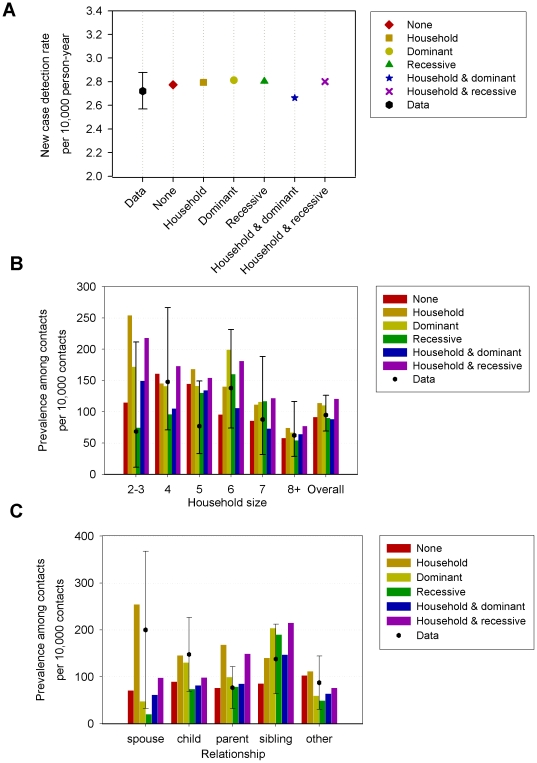
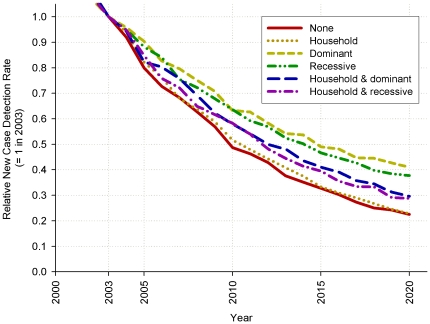
The epidemiology of leprosy is characterized by heterogeneity in susceptibility and clustering of disease within households. We aim to assess the extent to which different mechanisms for heterogeneity in leprosy susceptibility can explain household clustering as observed in a large study among contacts of leprosy patients.We used a microsimulation model, parameterizing it with data from over 20,000 contacts of leprosy patients in Bangladesh. We simulated six mechanisms producing heterogeneity in susceptibility: (1) susceptibility was allocated at random to persons (i.e. no additional mechanism), (2) a household factor, (3, 4) a genetic factor (dominant or recessive), or (5, 6) half a household factor and half genetic. We further assumed that a fraction of 5%, 10%, and 20% of the population was susceptible, leading to a total of 18 scenarios to be fitted to the data. We obtained an acceptable fit for each of the six mechanisms, thereby excluding none of the possible underlying mechanisms for heterogeneity of susceptibility to leprosy. However, the distribution of leprosy among contacts did differ between mechanisms, and predicted trends in the declining leprosy case detection were dependent on the assumed mechanism, with genetic-based susceptibility showing the slowest decline. Clustering of leprosy within households is partially caused by an increased transmission within households independent of the leprosy susceptibility mechanism. Even a large and detailed data set on contacts of leprosy patients could not unequivocally reveal the mechanism most likely responsible for heterogeneity in leprosy susceptibility.
Conflict of interest statement
Figures
References
-
- WHO. Global leprosy situation, 2009. Weekly Epidemiological Record. 2009;84:333–340.
-
- WHO. WHO Expert Committee on Leprosy. World Health Organ Tech Rep Ser. 1998;874:1–43. - PubMed
-
- Bakker MI, Hatta M, Kwenang A, Klatser PR, Oskam L. Epidemiology of leprosy on five isolated islands in the Flores Sea, Indonesia. Tropical Medicine & International Health. 2002;7:780–787. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
