

Tissue damage with different surgical techniques in a porcine model of liver resection: implications for living-donor liver transplantation?
- PMID: 21127914
- PMCID: PMC3291831
- DOI: 10.1007/s00534-010-0347-4
Tissue damage with different surgical techniques in a porcine model of liver resection: implications for living-donor liver transplantation?
Abstract
Background/purpose: For living-donor liver transplantation (LDLT) it is of paramount importance to preserve as much viable liver tissue as possible to avoid postoperative complications in the donor and recipient. The depth of tissue damage caused by common surgical techniques for liver resection has not been studied so far.
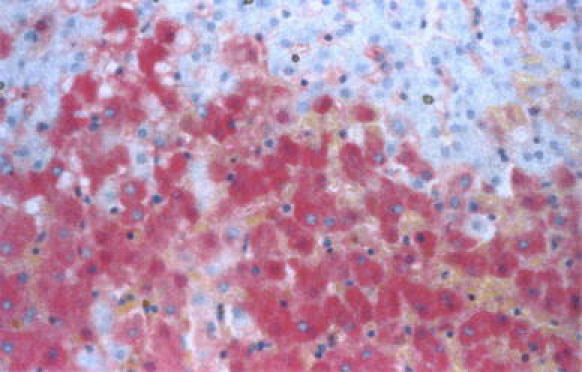
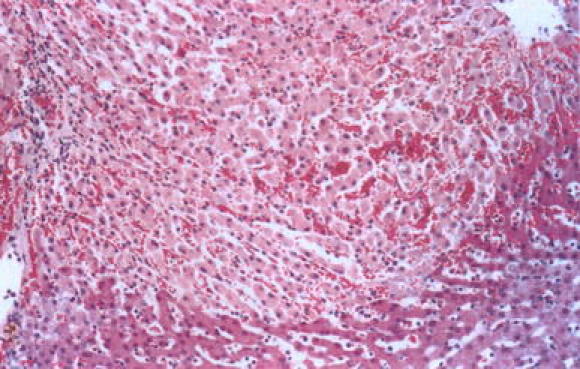
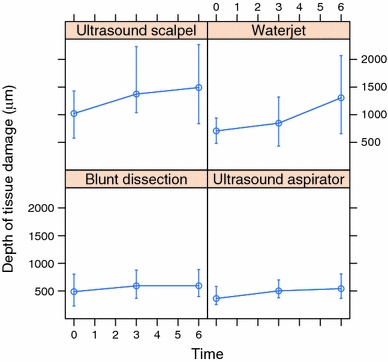
Methods: Here we compared the depth of tissue damage and the immunohistochemical expression of heat shock protein (HSP) 70, a marker for tissue damage, in a porcine model of liver resection, to assess the effect of different surgical techniques, i.e., blunt dissection (BD), and dissection with an ultrasound aspirator (UA), an ultrasound scalpel (US), or a water-jet (WJ).
Results: Analysis with linear mixed effects models (LME) showed significantly less tissue damage with BD and UA than with US and WJ (joint p value <0.001). Damage also increased within 6 h after surgery (p value = 0.004). Semiquantitative evaluation of HSP 70 showed increased expression after resection with US compared to all other resection methods (p value <0.001), indicating increased tissue damage with this method.
Conclusion: We suggest that in cases of liver resection for LDLT surgeons should reevaluate using US and WJ because of possible excessive tissue damage compared to BD and UA. Overall we advocate the use of BD as it requires no special equipment and, hence, has considerably higher cost-effectiveness without compromising tissue preservation and clinical outcome and is readily available even in low-tech environments.
Figures


Similar articles
-
Right lobe living donors ages 55 years old and older in liver transplantation.Liver Transpl. 2017 Oct;23(10):1305-1311. doi: 10.1002/lt.24823. Liver Transpl. 2017. PMID: 28734130
-
Living Donor Liver Transplantation for Acute Liver Failure: Donor Safety and Recipient Outcome.Liver Transpl. 2019 Sep;25(9):1408-1421. doi: 10.1002/lt.25445. Epub 2019 Jul 29. Liver Transpl. 2019. PMID: 30861306
-
Impact of intra-operative cholangiography and parenchymal resection to donor liver function in living donor liver transplantation.Hepatobiliary Pancreat Dis Int. 2014 Jun;13(3):259-63. doi: 10.1016/s1499-3872(14)60252-6. Hepatobiliary Pancreat Dis Int. 2014. PMID: 24919608
-
Hepatic Artery Reconstruction Using 3-in-1 Segmental Resection in Pediatric Living Donor Liver Transplantation: A Case Report and Literature Review.Transplant Proc. 2017 Sep;49(7):1619-1623. doi: 10.1016/j.transproceed.2017.01.076. Transplant Proc. 2017. PMID: 28838451 Review.
-
Liver resection and transplantation using a novel 3D hepatectomy simulation system.Adv Med Sci. 2006;51:7-14. Adv Med Sci. 2006. PMID: 17357270 Review.
Cited by
-
How to successfully resect 70 % of the liver in pigs to model an extended hepatectomy with an insufficient remnant or liver transplantation with a small-for-size graft.Surg Today. 2014 Nov;44(11):2201-7. doi: 10.1007/s00595-014-0862-z. Epub 2014 Feb 12. Surg Today. 2014. PMID: 24519397
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
