

Laparoscopic sleeve gastrectomy is a safe and effective bariatric procedure for the lower BMI (35.0-43.0 kg/m2) population
- PMID: 21128003
- PMCID: PMC3148435
- DOI: 10.1007/s11695-010-0332-7
Laparoscopic sleeve gastrectomy is a safe and effective bariatric procedure for the lower BMI (35.0-43.0 kg/m2) population
Abstract
Background: The laparoscopic vertical sleeve gastrectomy (LSG) is derived from the biliopancreatic diversion with duodenal switch operation (Marceau et al., Obes Surg 3:29-35, 1993; Hess and Hess, Obes Surg 8:267-82, 1998; Chu et al., Surg Endosc 16:S069, 2002). Later, LSG was advocated as the first step of a two-stage procedure for super-obese patients (Regan et al., Obes Surg 13:861-4, 2003; Cottam et al., Surg Endosc 20:859-63, 2006). However, recent support is mounting that continues to establish LSG as the definitive procedure for surgical treatment of morbid obesity. We will report our experience with the LSG as a primary bariatric procedure and evaluate if this operation is suitable as a stand-alone procedure.
Methods: The study is a nonrandomized retrospective analysis of 204 patients from a single surgeon operated between July 2006 and April 2010. The study comprises of 155 women and 49 men with a mean age of 45 years (range, 19-70 years), a mean preoperative weight of 126.6 kg, and body mass index (BMI) of 45.7 kg/m(2).
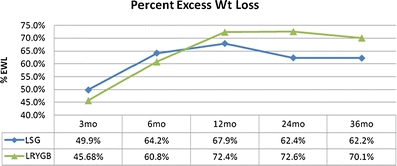
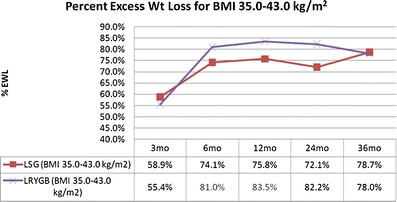
Results: The mean percent excess weight loss (%EWL) was 49.9% (n = 159), 64.2% (n = 138), 67.9% (n = 77), 62.4% (n = 34), and 62.2% (n = 9) at 3, 6, 12, 24, and 36 months, respectively. For patients with BMI ≤43.0, the mean postoperative %EWL was 58.9% (n = 72), 74.1% (n = 67), 75.8% (n = 39), 72.1% (n = 17), and 78.7% (n = 5) at 3, 6, 12, 24, and 36 months, respectively. Operative complications include leak (0.0%), abscess (0.5%), hemorrhage (1.0%), sleeve stricture (1.0%), and severe gastroesphogeal reflux disease with need to convert to laparoscopic Roux-en-Y gastric bypass (0.5%).
Conclusions: LSG yields excellent outcomes with low complication rates for morbidly obese patients. We advocate LSG as a safe and effective stand-alone procedure, especially with the lower BMI population (BMI 35.0-43.0 kg/m(2)).
Figures
References
-
- Chu CA, Gagner M, Quinn T, et al. Two-stage laparoscopic biliopancreatic diversion with duodenal switch: an alternative approach to super-super morbid obesity (abstract) Surg Endosc. 2002;16:S069.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
