

Scapular notching: Recognition and strategies to minimize clinical impact
- PMID: 21128030
- PMCID: PMC3148378
- DOI: 10.1007/s11999-010-1720-y
Scapular notching: Recognition and strategies to minimize clinical impact
Abstract
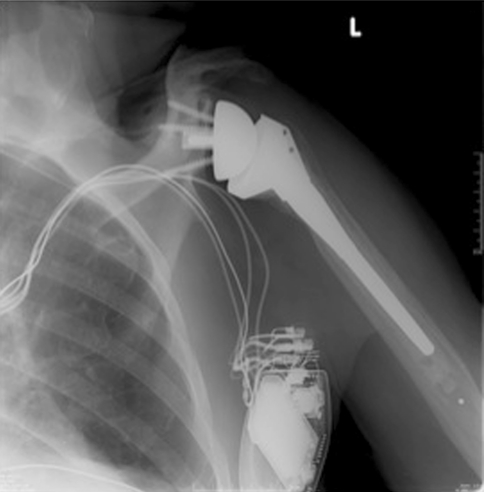
Background: Scapular notching is a unique complication of Grammont-style reverse total shoulder arthroplasty. While reverse total shoulder arthroplasty has revolutionized the treatment of pseudoparalysis secondary to cuff tear arthropathy, the implications of scapular notching with regard to patient function and implant stability remain unclear.
Questions/purposes: We reviewed literature to determine the etiology and incidence, radiographic progression and effect on implant stability, relationship with postoperative function, and risk factors for the development of scapular notching.
Methods: We reviewed PubMed, the Cochrane Central Register of Controlled Trials, and EMBASE with the terms "reverse total shoulder arthroplasty" and "scapular notching." Inclusion criteria were a level of evidence of IV (or better). Twenty-four articles were selected after manual review.
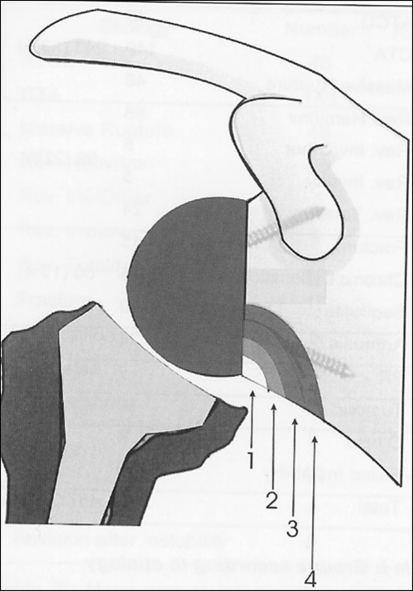
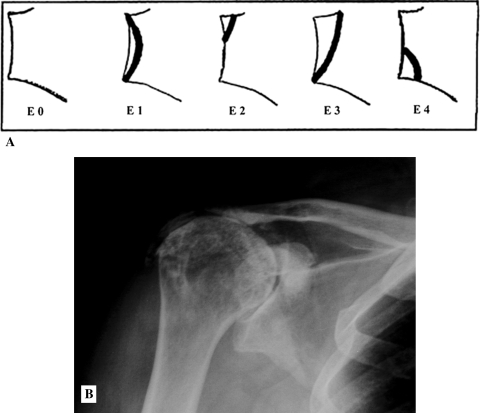
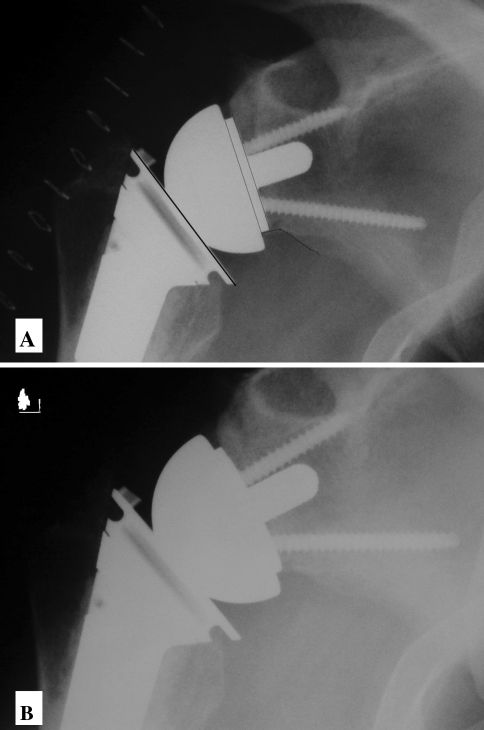
Results: Scapular notching after reverse total shoulder arthroplasty is due to repetitive contact between the polyethylene of the humeral component and the inferior scapular neck during adduction, leading to erosion of the scapular neck, polyethylene wear, joint inflammation, and potential implant loosening. Scapular notching appears between 6 and 14 months postoperatively, with an incidence of 44% to 96%. Radiographic progression and effect on patient function remain controversial. Predictors of scapular notching include surgical approach, glenoid wear, preoperative diagnosis, infraspinatus muscle quality, cranial-caudal positioning, and tilt of the glenosphere.
Conclusions: Improved understanding of the etiology and risk factors for scapular notching will lead to refinement in implant technology and surgical technique that may translate into improved patient function and implant longevity for Grammont-style reverse total shoulder arthroplasty.
Figures
References
-
- Boulahia A, Edwards TB, Walch G, Baratta RV. Early results of a reverse design prosthesis in the treatment of arthritis of the shoulder in elderly patients with a large rotator cuff tear. Orthopedics. 2002;25:129–133. - PubMed
-
- Delloye C, Joris D, Colette A, Eudier A, Dubuc JE. Mechanical complications of total shoulder inverted prosthesis [in French. Rev Chir Orthop Reparatrice Appar Mot. 2002;88:410–414. - PubMed
-
- Edwards TB, Boulahia A, Kempf JF, Boileau P, Nemoz C, Walch G. The influence of rotator cuff disease on the results of shoulder arthroplasty for primary osteoarthritis: results of a multicenter study. J Bone Joint Surg Am. 2002;84:2240–2248. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
