

Combining basal-bolus insulin infusion for tight postprandial glucose control: an in silico evaluation in adults, children, and adolescents
- PMID: 21129338
- PMCID: PMC3005053
- DOI: 10.1177/193229681000400617
Combining basal-bolus insulin infusion for tight postprandial glucose control: an in silico evaluation in adults, children, and adolescents
Abstract
Background: Achieving good postprandial glycemic control, without triggering hypoglycemia events, is a challenge of treatment strategies for type 1 diabetes subjects. Continuous subcutaneous insulin infusion, the gold standard of therapy, is based on heuristic adjustments of both basal and prandial insulin. Some tools, such as bolus calculators, are available to aid patients in selecting a meal-related insulin dose. However, they are still based on empiric parameters such as the insulin-to-carbohydrate ratio and on the physicians' and patients' ability to fit bolus mode to meal composition.
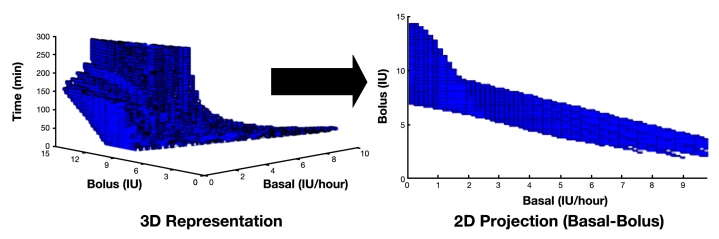
Methods: In this article, a nonheuristic method for assessment of prandial insulin administration is presented and evaluated. An algorithm based on set inversion via interval analysis is used to coordinate basal and bolus insulin infusions to deal with postprandial glucose excursions. The evaluation is carried out through an in silico study using the 30 virtual patients available in the educational version of the Food and Drug Administration-accepted University of Virginia simulator. Results obtained using the standard bolus strategy and different coordinated basal-bolus solutions provided by the algorithm are compared.
Results: Coordinated basal-bolus solutions improve postprandial glucose performance in most cases, mainly in terms of reducing hypoglycemia risk, but also increasing the percentage of time in normoglycemia. Moreover, glycemic variability is reduced considerably by using these innovative solutions.
Conclusions: The algorithm presented here is a robust nonheuristic alternative to deal with postprandial glycemic control. It is shown as a powerful tool that could be integrated in future smart insulin pumps.
© 2010 Diabetes Technology Society.
Figures






References
-
- The Diabetes Control and Complications Trial Research Group The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977–986. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352(9131):837–853. - PubMed
-
- Gresele P, Guglielmini G, De Angelis M, Ciferri S, Ciofetta M, Falcinelli E, Lalli C, Ciabattoni G, Davi G, Bolli G B. Acute, short-term hyperglycemia enhances shear stress-induced platelet activation in patients with type II diabetes mellitus. J Am Coll Cardiol. 2003;41(6):1013–1020. - PubMed
-
- Zaccardi F, Pitocco D, Ghirlanda G. Glycemic risk factors of diabetic vascular complications: the role of glycemic variability. Diabetes Metab Res Rev. 2009;25(3):199–207. - PubMed
-
- Monnier L, Colette C, Dunseath GJ, Owens DR. The loss of postprandial glycemic control precedes stepwise deterioration of fasting with worsening diabetes. Diabetes Care. 2007;30(2):263–269. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
