

Translation of personalized decision support into routine diabetes care
- PMID: 21129352
- PMCID: PMC3005067
- DOI: 10.1177/193229681000400631
Translation of personalized decision support into routine diabetes care
Abstract
Objective: The aim of this study was to evaluate the impact of personalized decision support (PDS) on metabolic control in people with diabetes and cardiovascular disease.
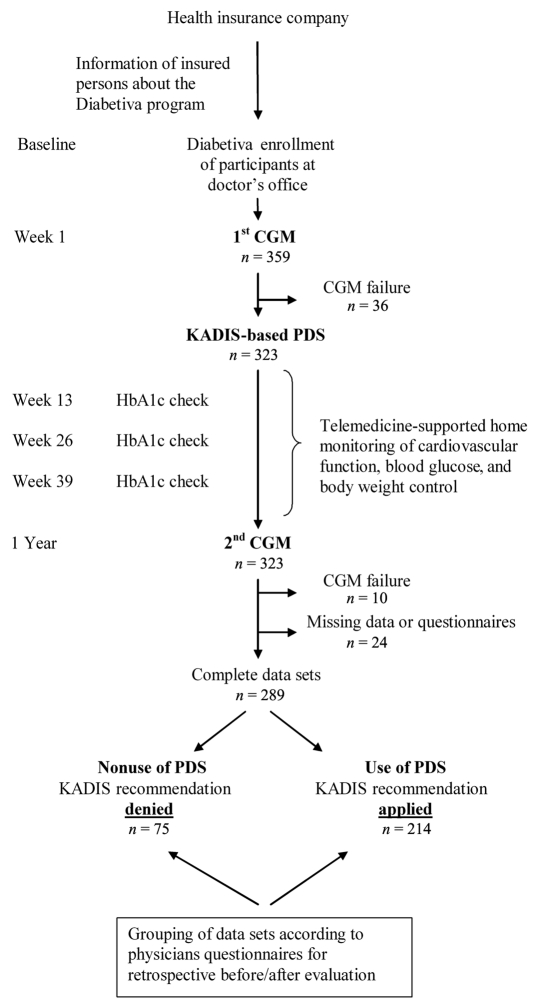
Research design and methods: The German health insurance fund BKK TAUNUS offers to its insured people with diabetes and cardiovascular disease the possibility to participate in the Diabetiva® program, which includes PDS. Personalized decision support is generated by the expert system KADIS® using self-control data and continuous glucose monitoring (CGM) as its data source. The physician of the participating person receives the PDS once a year, decides about use or nonuse, and reports his/her decision in a questionnaire. Metabolic control of participants treated by use or nonuse of PDS for one year and receiving CGM twice was analyzed in a retrospective observational study. The primary outcome was hemoglobin A1c (HbA1c); secondary outcomes were mean sensor glucose (MSG), glucose variability, and hypoglycemia.
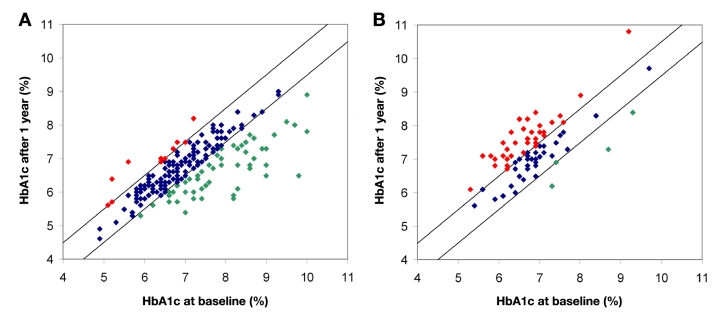
Results: A total of 323 subjects received CGM twice, 289 had complete data sets, 97% (280/289) were type 2 diabetes patients, and 74% (214/289) were treated using PDS, resulting in a decrease in HbA1c [7.10±1.06 to 6.73±0.82%; p<.01; change in HbA1ct0-t12 months -0.37 (95% confidence interval -0.46 to -0.28)] and MSG (7.7±1.6 versus 7.4±1.2 mmol/liter; p=.003) within one year. Glucose variability was also reduced, as indicated by lower high blood glucose index (p=.001), Glycemic Risk Assessment Diabetes Equation (p=.009), and time of hyper-glycemia (p=.003). Low blood glucose index and time spent in hypoglycemia were not affected. In contrast, nonuse of PDS (75/289) resulted in increased HbA1c (p<.001). Diabetiva outcome was strongly related to baseline HbA1c (HbA1ct0; p<.01) and use of PDS (p<.01). Acceptance of PDS was dependent on HbA1ct0 (p=.049).
Conclusions: Personalized decision support has potential to improve metabolic outcome in routine diabetes care.
© 2010 Diabetes Technology Society.
Figures

References
-
- Augstein P, Vogt L, Kohnert KD, Freyse EJ, Heinke P, Salzsieder E. Outpatient assessment of Karlsburg Diabetes Management System-based decision support. Diabetes Care. 2007;30(7):1704–1708. - PubMed
-
- Rutscher A, Salzsieder E, Thierbach U, Fischer U, Albrecht G. KADIS—a computer-aided decision support system for improving the management of type-I diabetes. Exp Clin Endocrinol. 1990;95(1):137–147. - PubMed
-
- Birati EY, Malov N, Kogan Y, Yanay Y, Tamari M, Elizur M, Steinberg DM, Golovner M, Roth A. Vigilance, awareness and a phone line: 20 years of expediting CPR for enhancing survival after out-of-hospital cardiac arrest The ‘SHL’-Telemedicine experience in Israel. Resuscitation. 2008;79(3):438–443. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
