

Lymph node ratio as a prognostic factor in elderly patients with pathological N1 non-small cell lung cancer
- PMID: 21131298
- PMCID: PMC5642294
- DOI: 10.1136/thx.2010.148601
Lymph node ratio as a prognostic factor in elderly patients with pathological N1 non-small cell lung cancer
Abstract
Background: Lymph node (LN) metastasis is an important predictor of survival for patients with non-small cell lung cancer (NSCLC). However, the prognostic significance of the extent of LN involvement among patients with N1 disease remains unknown. A study was undertaken to evaluate whether involvement of a higher number of N1 LNs is associated with worse survival independent of known prognostic factors.
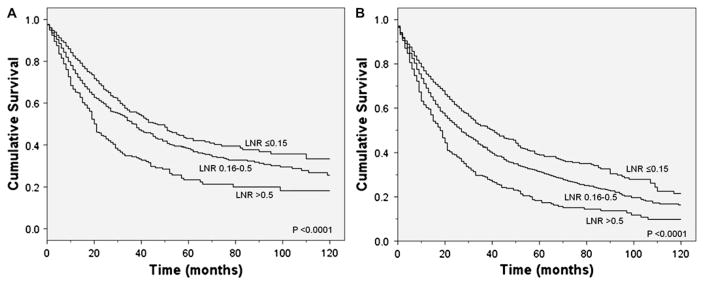
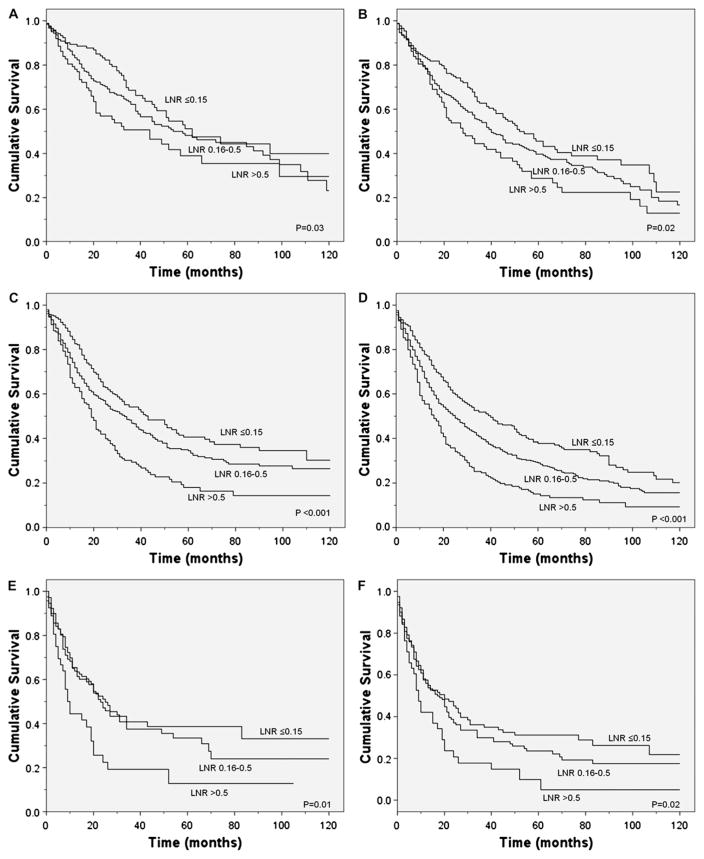
Methods: Using the Surveillance, Epidemiology and End Results-Medicare database, 1682 resected patients with N1 NSCLC diagnosed between 1992 and 2005 were identified. As the number of positive LNs is confounded by the total number of LNs sampled, the cases were classified into three groups according to the ratio of positive to total number of LNs removed (LN ratio (LNR)): ≤0.15, 0.16-0.5 and >0.5. Lung cancer-specific and overall survival was compared between these groups using Kaplan-Meier curves. Stratified and Cox regression analyses were used to evaluate the relationship between the LNR and survival after adjusting for potential confounders.
Results: Lung cancer-specific and overall survival was lower among patients with a high LNR (p<0.0001 for both comparisons). Median lung cancer-specific survival was 47 months, 37 months and 21 months for patients in the ≤0.15, 0.16-0.5 and >0.5 LNR groups, respectively. In stratified and adjusted analyses, a higher LNR was also associated with worse lung cancer-specific and overall survival.
Conclusions: The extent of LN involvement provides independent prognostic information in patients with N1 NSCLC. This information may be used to identify patients at high risk of recurrence who may benefit from aggressive postoperative therapy.
Conflict of interest statement
Figures
Comment in
-
Quantification of regional lymph node involvement in lung cancer.Thorax. 2011 Apr;66(4):271-2. doi: 10.1136/thx.2010.155010. Thorax. 2011. PMID: 21422042 No abstract available.
-
Imaging in lung cancer: recent advances in PET-CT and screening.Thorax. 2011 Apr;66(4):275-7. doi: 10.1136/thx.2010.149153. Thorax. 2011. PMID: 21422043 No abstract available.
Similar articles
-
Validation of the lymph node ratio as a prognostic factor in patients with N1 nonsmall cell lung cancer.Cancer. 2011 Oct 15;117(20):4724-31. doi: 10.1002/cncr.26093. Epub 2011 Mar 30. Cancer. 2011. PMID: 21452193 Free PMC article.
-
The number of lymph node metastases as a prognostic factor in patients with N1 non-small cell lung cancer.Chest. 2011 Aug;140(2):433-440. doi: 10.1378/chest.10-2885. Epub 2011 Feb 3. Chest. 2011. PMID: 21292754 Free PMC article.
-
Log odds of positive lymph nodes may predict survival benefit in patients with node-positive non-small cell lung cancer.Lung Cancer. 2018 Aug;122:60-66. doi: 10.1016/j.lungcan.2018.05.016. Epub 2018 May 23. Lung Cancer. 2018. PMID: 30032846
-
Prognostic significance of the extent of lymph node involvement in stage II-N1 non-small cell lung cancer.Chest. 2013 Oct;144(4):1253-1260. doi: 10.1378/chest.13-0073. Chest. 2013. PMID: 23744276
-
Value of the metastatic lymph node ratio for predicting the prognosis of non-small-cell lung cancer patients.World J Surg. 2012 Feb;36(2):455-62. doi: 10.1007/s00268-011-1360-8. World J Surg. 2012. PMID: 22187129
Cited by
-
Pattern of lymph node metastases and its implication in radiotherapeutic clinical target volume in patients with non-small-cell lung cancer: a study of 2062 cases.Br J Radiol. 2015;88(1056):20140288. doi: 10.1259/bjr.20140288. Epub 2015 Jun 30. Br J Radiol. 2015. PMID: 26126020 Free PMC article.
-
Lymph node ratio predicts overall survival in patients with stage II non-small cell lung cancer: a population-based SEER analysis.Discov Oncol. 2022 Aug 18;13(1):75. doi: 10.1007/s12672-022-00542-w. Discov Oncol. 2022. PMID: 35982330 Free PMC article.
-
Lymph Node Ratio Rather Than Positive Lymph Node Counts Has Better Prognostic Value in Patients With Testicular Germ Cell Tumors.Technol Cancer Res Treat. 2021 Jan-Dec;20:1533033820979702. doi: 10.1177/1533033820979702. Technol Cancer Res Treat. 2021. PMID: 33455540 Free PMC article.
-
Prognostic impact of lymph node ratio in patients with pT1-2N1M0 non-small cell lung cancer.J Thorac Dis. 2020 Oct;12(10):5552-5560. doi: 10.21037/jtd-20-1611. J Thorac Dis. 2020. PMID: 33209388 Free PMC article.
-
Reduced impact of nodal metastases as a prognostic factor for tonsil cancer in the HPV era.Eur Arch Otorhinolaryngol. 2014 Sep;271(9):2523-9. doi: 10.1007/s00405-013-2796-2. Epub 2013 Nov 5. Eur Arch Otorhinolaryngol. 2014. PMID: 24190760 Free PMC article.
References
-
- Mountain CF, Dresler CM. Regional lymph node classification for lung cancer staging. Chest. 1997;111:1718–23. - PubMed
-
- Tanaka F, Yanagihara K, Otake Y, et al. Prognostic factors in patients with resected pathologic (p-) T1-2N1M0 non-small cell lung cancer (NSCLC) Eur J Cardiothorac Surg. 2001;19:555–61. - PubMed
-
- van Rens MT, de la Riviere AB, Elbers HR, et al. Prognostic assessment of 2,361 patients who underwent pulmonary resection for non-small cell lung cancer, stage I, II, and IIIA. Chest. 2000;117:374–9. - PubMed
-
- van Velzen E, Snijder RJ, Brutel de la Riviere A, et al. Lymph node type as a prognostic factor for survival in T2 N1 M0 non-small cell lung carcinoma. Ann Thorac Surg. 1997;63:1436–40. - PubMed
-
- Martini N, Flehinger BJ, Nagasaki F, et al. Prognostic significance of N1 disease in carcinoma of the lung. J Thorac Cardiovasc Surg. 1983;86:646–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials