

Endocardial unipolar voltage mapping to detect epicardial ventricular tachycardia substrate in patients with nonischemic left ventricular cardiomyopathy
- PMID: 21131557
- PMCID: PMC3041847
- DOI: 10.1161/CIRCEP.110.959957
Endocardial unipolar voltage mapping to detect epicardial ventricular tachycardia substrate in patients with nonischemic left ventricular cardiomyopathy
Abstract
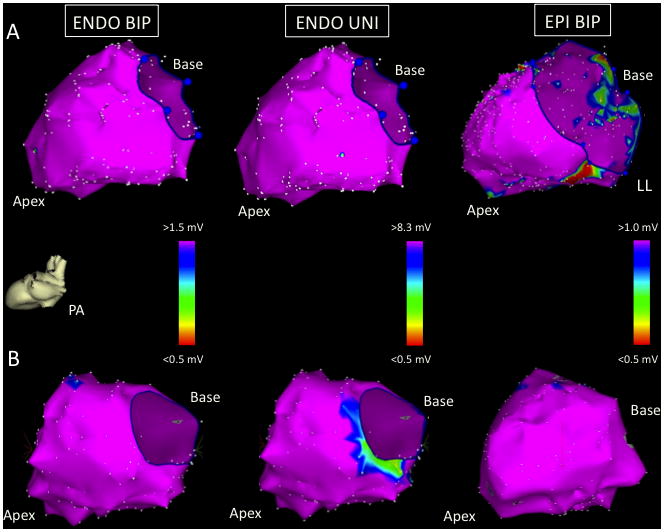
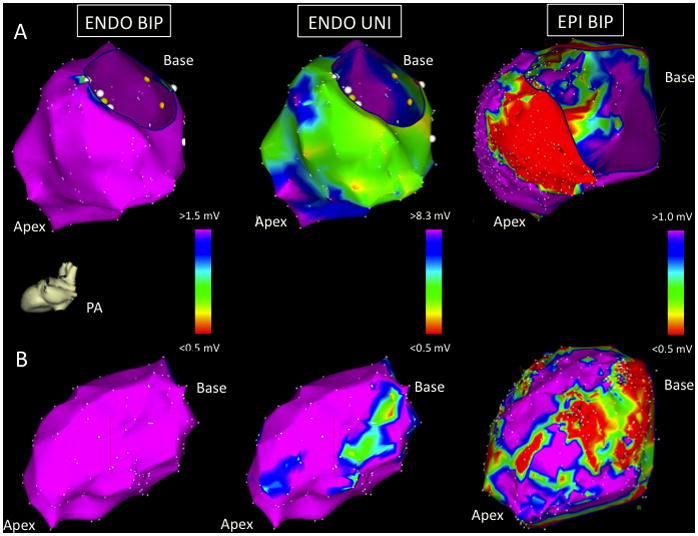
Background: Patients with nonischemic left ventricular cardiomyopathy (LVCM) and ventricular tachycardia (Vt) have complex 3-dimensional substrate with variable involvement of the endocardium (ENDO) and epicardium (EPI). The purpose of this study was to determine whether ENDO unipolar (UNI) mapping with a larger electric field of view could identify EPI low bipolar (BIP) voltage regions in patients with LVCM undergoing Vt ablation.
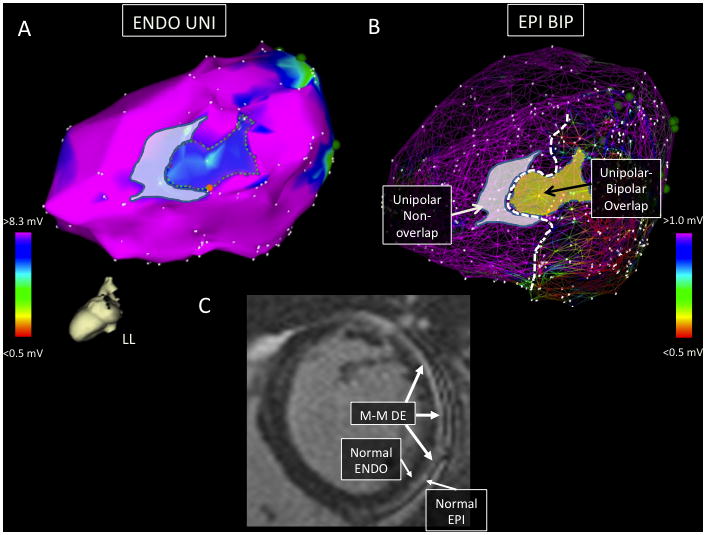
Methods and results: The reference value for normal ENDO unipolar voltage was determined from 6 patients without structural heart disease. Consecutive patients undergoing Vt ablation over an 8-year period with detailed (>100 points) LV ENDO and EPI mapping and normal LV ENDO BIP voltage were identified. From this cohort, we compared patients with structurally normal hearts and normal EPI BIP voltage (EPI-, group 1) with patients with LVCM and low LV EPI BIP voltage regions present (EPI+, group 2). Confluent regions of ENDO UNI and EPI BIP low voltage (>2 cm(2)) were measured. The normal signal amplitude was >8.27 mV for LV ENDO UNI electrograms. Detailed LV ENDO-EPI maps in 5 EPI- patients were compared with 11 EPI+ patients. Confluent ENDO UNI low-voltage regions were seen in 9 of 11 (82%) of the EPI+ (group 2) patients compared with none of 5 EPI- (group 1) patients (P<0.001). In all 9 patients with ENDO UNI low voltage, the ENDO UNI low-voltage regions were directly opposite to an area of EPI BIP low voltage (61% ENDO UNI-EPI BIP low-voltage area overlap).
Conclusions: EPI arrhythmia substrate can be reliably identified in most patients with LVCM using ENDO UNI voltage mapping in the absence of ENDO BIP abnormalities.
Figures
References
-
- Hsia HH, Callans DJ, Marchlinski FE. Characterization of endocardial electrophysiological substrate in patients with nonischemic cardiomyopathy and monomorphic ventricular tachycardia. Circulation. 2003;108:704–710. - PubMed
-
- Soejima K, Stevenson WG, Sapp JL, Selwyn AP, Couper G, Epstein LM. Endocardial and epicardial radiofrequency ablation of ventricular tachycardia associated with dilated cardiomyopathy: the importance of low-voltage scars. J Am Coll Cardiol. 2004;43:1834–1842. - PubMed
-
- Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation. 2000;101:1288–1296. - PubMed
-
- Delacretaz E, Stevenson WG, Ellison KE, Maisel WH, Friedman PL. Mapping and radiofrequency catheter ablation of the three types of sustained monomorphic ventricular tachycardia in nonischemic heart disease. J Cardiovasc Electrophysiol. 2000;11:11–17. - PubMed
-
- Cano O, Hutchinson M, Lin D, Garcia F, Zado E, Bala R, Riley M, Cooper J, Dixit S, Gerstenfeld E, Callans D, Marchlinski FE. Electroanatomic substrate and ablation outcome for suspected epicardial ventricular tachycardia in left ventricular nonischemic cardiomyopathy. J Am Coll Cardiol. 2009;54:799–808. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
