

Reduction in physician reimbursement and use of hormone therapy in prostate cancer
- PMID: 21131577
- PMCID: PMC3001964
- DOI: 10.1093/jnci/djq417
Reduction in physician reimbursement and use of hormone therapy in prostate cancer
Abstract
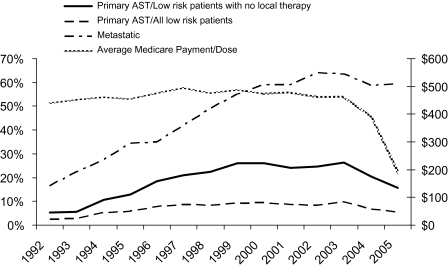
Background: Use of androgen suppression therapy (AST) in prostate cancer increased more than threefold from 1991 to 1999. The 2003 Medicare Modernization Act reduced reimbursements for AST by 64% between 2004 and 2005, but the effect of this large reduction on use of AST is unknown.
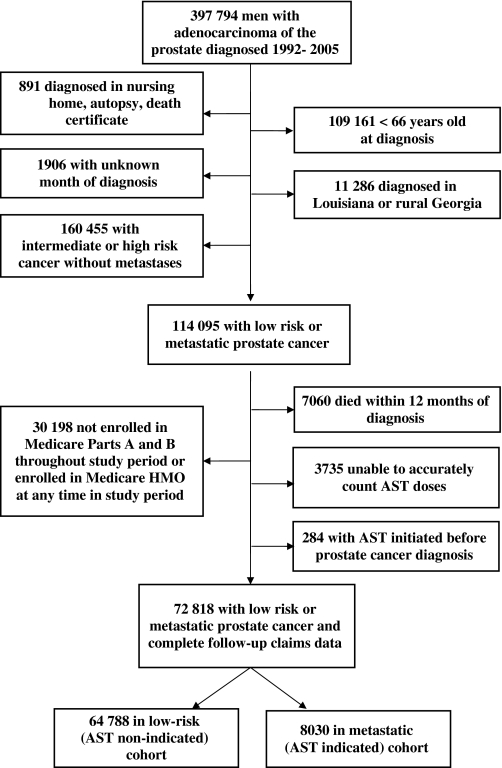
Methods: A cohort of 72,818 men diagnosed with prostate cancer in 1992-2005 was identified from the Surveillance, Epidemiology, and End Results database. From Medicare claims data, indicated AST was defined as 3 months or more of AST in the first year in men with metastatic disease (n = 8030). Non-indicated AST was defined as AST given without other therapies such as radical prostatectomy or radiation in men with low-risk disease (n = 64,788). The unadjusted annual proportion of men receiving AST was plotted against the median Medicare AST reimbursement. A multivariable model was used to estimate the odds of AST use in men with low-risk and metastatic disease, with the predictor of interest being the calendar year of the payment change. Covariates in the model included age in 5-year categories, clinical tumor stage (T1-T4), World Health Organization grade (1-3, unknown), Charlson comorbidity (0, 1, 2, ≥ 3), race, education, income, and tumor registry site, all as categorical variables. The models included variations in the definition of AST use (≥ 1, ≥ 3, and ≥ 6 months of AST). All statistical tests were two-sided.
Results: AST use in the low-risk group peaked at 10.2% in 2003, then declined to 7.1% in 2004 and 6.1% in 2005. After adjusting for tumor and demographic covariates, the odds of receiving non-indicated primary AST decreased statistically significantly in 2004 (odds ratio [OR] = 0.70, 95% confidence interval = 0.61 to 0.80) and 2005 (OR = 0.61, 95% confidence interval = 0.53 to 0.71) compared with 2003. AST use in the metastatic disease group was stable at 60% during the payment change, and the adjusted odds ratio of receiving AST in this group was unchanged in 2004-2005.
Conclusions: In this example of hormone therapy for prostate cancer, decreased physician reimbursement was associated with a reduction in overtreatment without a reduction in needed services.
Figures
Comment in
-
Medicare reimbursement and prescribing hormone therapy for prostate cancer.J Natl Cancer Inst. 2010 Dec 15;102(24):1814-5. doi: 10.1093/jnci/djq467. Epub 2010 Dec 3. J Natl Cancer Inst. 2010. PMID: 21131579 No abstract available.
References
-
- Horsely S. “Obama: Overtreatment drives health care costs.”. All Things Considered on National Public Radio. July 21, 2009. http://www.npr.org/templates/story/story.php?storyId=106859968.
-
- Brownlee S. Overtreated: Why Too Much Medicine is Making us Sicker and Poorer. 1st U.S. ed. New York, NY: Bloomsbury: Distributed to the trade by Holtzbrinck Publishers; 2007.
-
- Gawande A. The cost conundrum. The New Yorker 2009. June 1, 2009
-
- Arrow K. Uncertainty and the welfare economics of medical care. Am Econ Rec. 1963;53:941–973.
-
- Wennberg JE, Cooper MM. Dartmouth Atlas of Health Care. Chicago, IL: American Hospital Publishing; 1996. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
