

A randomized-controlled trial of computerized alerts to reduce unapproved medication abbreviation use
- PMID: 21131606
- PMCID: PMC3005872
- DOI: 10.1136/jamia.2010.006130
A randomized-controlled trial of computerized alerts to reduce unapproved medication abbreviation use
Abstract
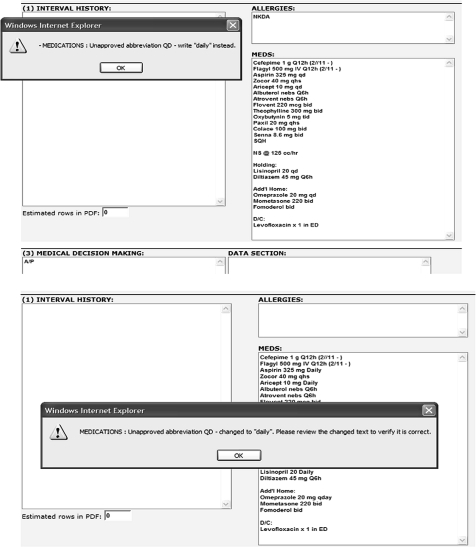
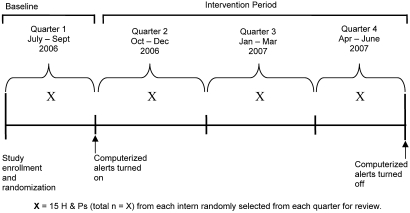
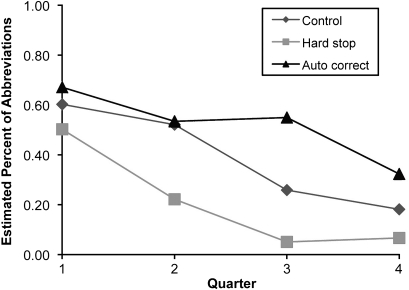
Abbreviation use is a preventable cause of medication errors. The objective of this study was to test whether computerized alerts designed to reduce medication abbreviations and embedded within an electronic progress note program could reduce these abbreviations in the non-computer-assisted handwritten notes of physicians. Fifty-nine physicians were randomized to one of three groups: a forced correction alert group; an auto-correction alert group; or a group that received no alerts. Over time, physicians in all groups significantly reduced their use of these abbreviations in their handwritten notes. Physicians exposed to the forced correction alert showed the greatest reductions in use when compared to controls (p=0.02) and the auto-correction alert group (p=0.0005). Knowledge of unapproved abbreviations was measured before and after the intervention and did not improve (p=0.81). This work demonstrates the effects that alert systems can have on physician behavior in a non-computerized environment and in the absence of knowledge.
Conflict of interest statement
Figures
References
-
- Kohn LT, Corrigan JM, Donaldson MS. To Err is Human: Building a Safer Health System. Washington, DC: (US) Committee on Quality of Health Care in America, Institute of Medicine, National Academy Press, 2000 - PubMed
-
- Lesar TS, Briceland L, Stein DS. Factors related to errors in medication prescribing. JAMA 1997;277:312–17 - PubMed
-
- Barker KN, Flynn EA, Pepper GA, et al. Medication errors observed in 36 healthcare facilities. Arch Intern Med 2002;162:1897–903 - PubMed
-
- The Joint Commission Accreditation Program: Hospital National Patient Safety Goals. NPSG 02.02.01 accessed at http://www.jointcommission.org/NR/rdonlyres/31666E86-E7F4-423E-9BE8-F05B... page 5 on 8 Jun 2009.
-
- ISMP and FDA Campaign to eliminate use of error-prone abbreviations. http://www.ismp.org/tools/abbreviations (accessed 8 Jun 2009).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
