

Pharmacogenetics of intravenous and oral busulfan in hematopoietic cell transplant recipients
- PMID: 21135089
- PMCID: PMC3117932
- DOI: 10.1177/0091270010382915
Pharmacogenetics of intravenous and oral busulfan in hematopoietic cell transplant recipients
Abstract
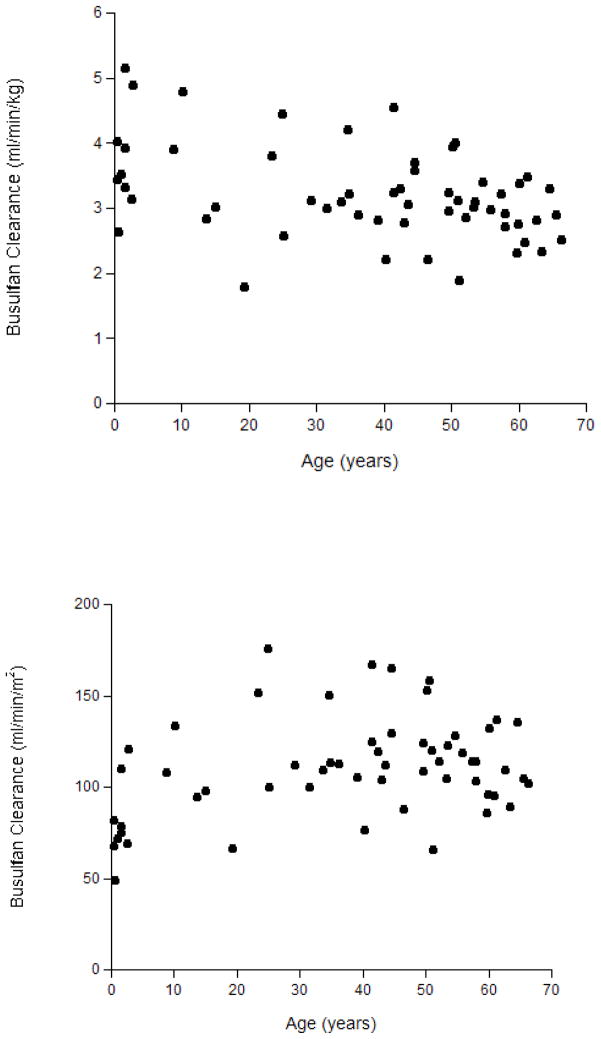
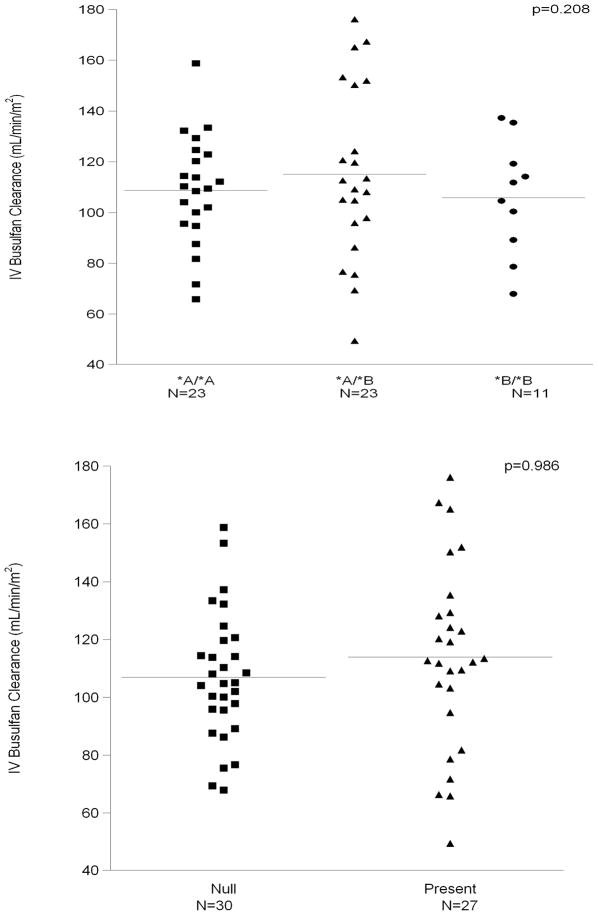
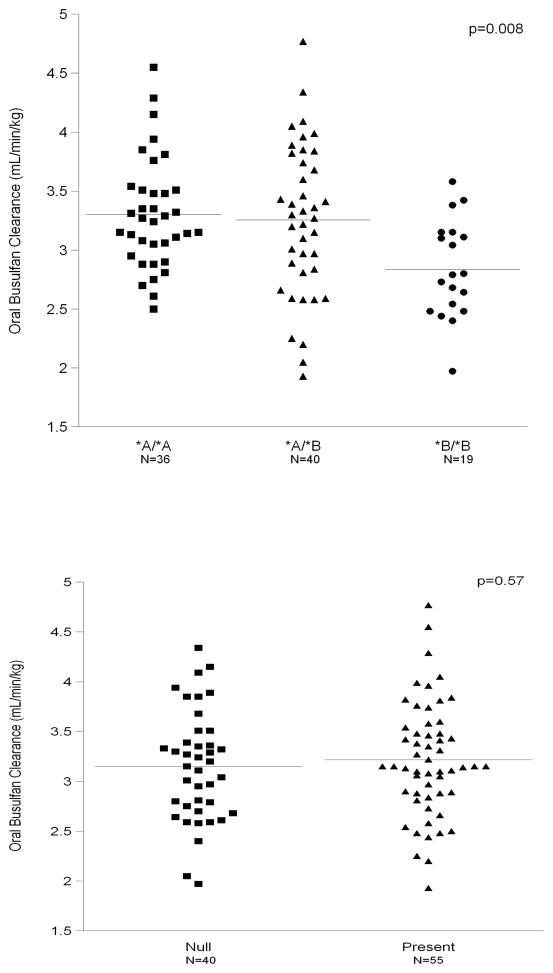
Kinetics-based dose targeting is often conducted in hematopoietic cell transplant (HCT) patients conditioned with intravenous (IV) or oral busulfan to lower rates of rejection, nonrelapse mortality, and relapse. Using the candidate gene approach, the authors evaluated whether busulfan clearance was associated with polymorphisms in the genes regulating the predominant metabolizing enzymes involved in busulfan conjugation, specifically glutathione S-transferase (GST) isoenzymes A1 (GSTA1) and M1 (GSTM1). Busulfan clearance was estimated after the morning dose on days 1, 2, and 3; each patient's average clearance was used for analyses. The average (± standard deviation) busulfan clearance was 3.2 ± 0.56 mL/min/kg in the separate population of 95 patients who received oral busulfan and 103 ± 24 ml/min/m(2) in the 57 patients who received IV busulfan. Oral busulfan clearance was associated with GSTA1 (P = .008) but not GSTM1 (P = .57) genotypes. However, among the GSTA1 haplotypes (ie, *A*A, *A*B, *B*B), there was significant overlap in the observed oral busulfan clearance and similar rates of achieving the target busulfan exposure. Clearance of IV busulfan was not associated with GSTA1 (P = .21) or GSTM1 (P = .99). These data suggest that personalizing either IV or oral busulfan dosing cannot be simplified on the basis of GSTA1 or GSTM1 genotype.
Figures
References
-
- Deeg HJ, Maris MB, Scott BL, Warren EH. Optimization of allogeneic transplant conditioning: not the time for dogma. Leukemia. 2006 Oct;20(10):1701–1705. - PubMed
-
- McCune JS, Gibbs JP, Slattery JT. Plasma concentration monitoring of busulfan: does it improve clinical outcome? Clin Pharmacokinet. 2000;39(2):155–165. - PubMed
-
- Field T, Perkins J, Alsina M, et al. Busulfan Area-under-the-Curve Finding Study within a Busulfan/Fludarabine (BuFlu) Conditioning Regimen before Allogeneic Hematopoietic Cell Transplantation (HCT) Blood. 2006 November 16;108(11) abstract #2939.
-
- Undevia SD, Gomez-Abuin G, Ratain MJ. Pharmacokinetic variability of anticancer agents. Nat Rev Cancer. 2005 Jun;5(6):447–458. - PubMed
-
- Deeg HJ, Storer BE, Boeckh M, et al. Reduced incidence of acute and chronic graft-versus-host disease with the addition of thymoglobulin to a targeted busulfan/cyclophosphamide regimen. Biol Blood Marrow Transplant. 2006 May;12(5):573–584. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
