

Review
. 2010 Dec 7;122(23):2430-40; discussion 2440.
doi: 10.1161/CIRCULATIONAHA.110.978924.
Genetics and clinical destiny: improving care in hypertrophic cardiomyopathy
Affiliations
- PMID: 21135371
- PMCID: PMC3100192
- DOI: 10.1161/CIRCULATIONAHA.110.978924
Item in Clipboard
Review
Genetics and clinical destiny: improving care in hypertrophic cardiomyopathy
Circulation.
.
No abstract available
Figures
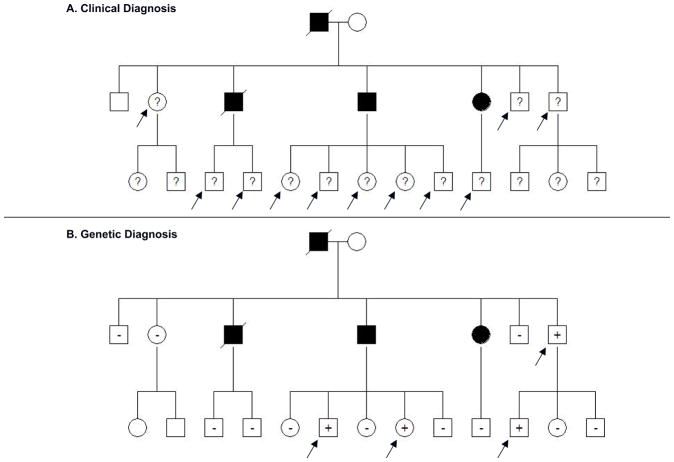
A. Pedigree of a family with HCM: Clinical screening is recommended for first degree relatives of patients with HCM to identify people with left ventricular hypertrophy and previously unrecognized disease. In this example, at least 11 family members (arrows) without LVH and of unknown genotype (?) are at risk for developing HCM and require longitudinal clinical evaluation. B. With genetic testing, serial clinical screening can be appropriately focused on mutation carriers, since relatives who have not inherited the pathogenic mutation are not at risk for disease development. In this family, only the 4 mutation carriers without clinical HCM (arrows) would require longitudinal follow up to assess for disease onset. Circles, females; squares males; solid symbols, clinical diagnosis of HCM; slash, deceased; ?, genotype unknown; +, mutation present; −, mutation absent
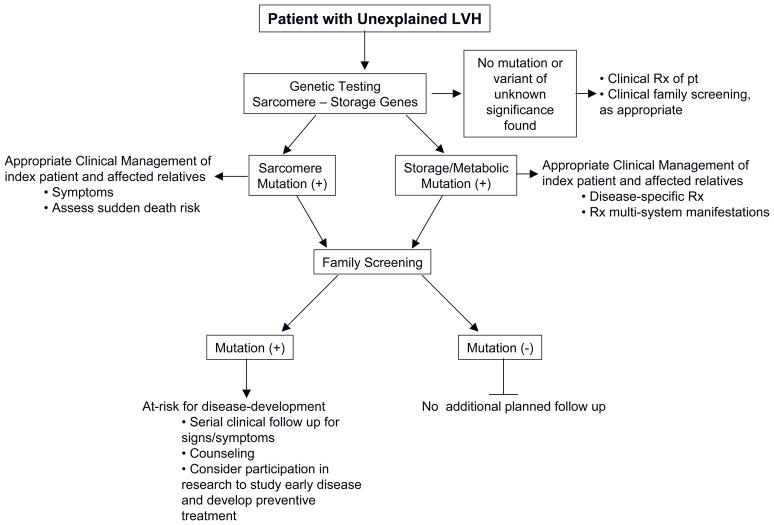
A general framework for incorporating genetic testing in the approach to patients and families with unexplained LVH.
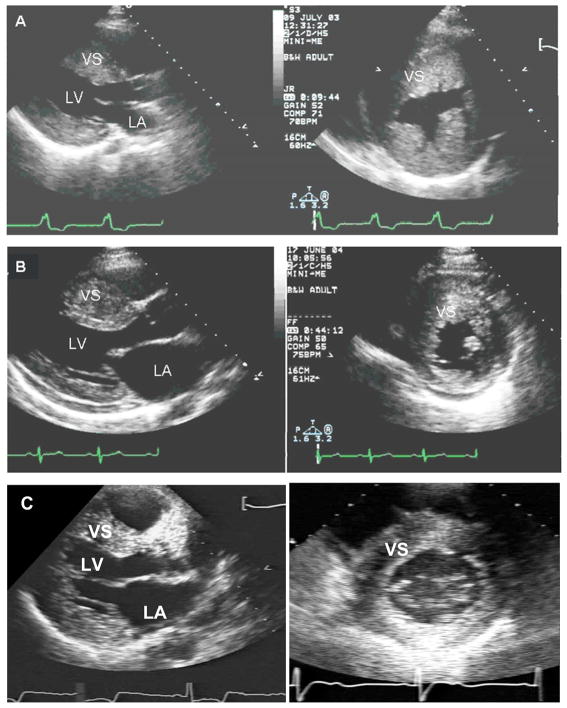
A. Parasternal long and short axis echocardiographic images from an 18 year-old male with a LAMP2 mutation. There is marked, diffuse LV hypertrophy with a maximal LV septal wall thickness of 35 mm. B. Parasternal images from a 20 year old female with a myosin heavy chain (MYH7) mutation, also showing marked, diffuse LVH, with a maximal wall thickness of 30 mm. By imaging alone, these patients cannot be discriminated although his disease course is predicted to be quite different, with a considerably worse prognosis in patient A. C. Parasternal images from a 45 year-old male with a GLA mutation and cardiac-restricted Fabry disease. Maximal septal wall thickness is 22 mm. LV= left ventricle; LA= left atrium; VS= ventricular septum
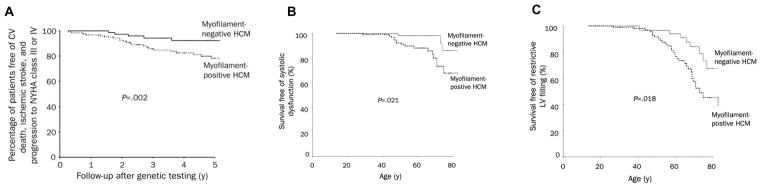
A. Myofilament-positive patients have a higher probability of cardiovascular (CV) death, nonfatal ischemic stroke, or progression to severe heart failure symptoms (New York Health Association (NYHA) functional classes III or IV). B. Myofilament-positive patients have a higher probability of developing systolic dysfunction, defined as LV ejection fraction <50%. C. Myofilament-positive patients have a higher probability of developing restrictive LV filling pattern, defined as transmitral early deceleration time <120 ms or a ratio of peak mitral early to late diastolic filling velocity (E/A ratio) of ≥ 2 in conjunction with a deceleration time of ≥ 150 ms. Adapted with permission from Olivotto I. et al. Mayo Clinic proceedings 2008;83(6):630–8.
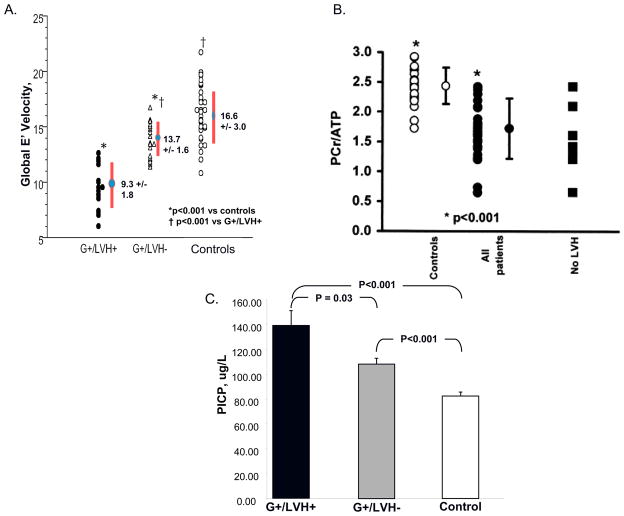
A. Impaired relaxation is detectable as reduced early myocardial relaxation velocities (E′) on tissue Doppler interrogation in mutation carriers who have not yet developed LVH (G+/LVH−) compared to normal controls. E′ velocities fall further with the development of overt HCM (G+/LVH+). Adapted with permission from Ho CY, et al. Circulation 2002;105(25):2992–7. B. Mutation carriers have impaired myocardial energetics as manifest by decreased Phosphocreatine/adenosine triphosphate (PCr/ATP) ratio. This is present all patients, including mutation carriers without LVH. Filled circles, HCM patients; open circles, controls; filled squares, mutation carriers without LVH. Adapted with permission from Crilley JG, et al. Journal of the American College of Cardiology 2003;41(10):1776–82. C. Mutation carriers show evidence of increased collagen synthesis, as manifest by increased serum levels of C-terminal propeptide of type I procollagen (PICP), before LVH develops (G+/LVH+). Compared to controls, PICP levels are significantly increased in all sarcomere mutations carriers, with (G+/LVH+) and without (G+/LVH−) hypertrophy. The threshold for significance is P <0.017 and adjusted for age and family relations. Reproduced with permission from Ho, C.Y., et al, N Engl J Med 2010;363(6):552–563.
Comment in
-
Mutation type is not clinically useful in predicting prognosis in hypertrophic cardiomyopathy.Circulation. 2010 Dec 7;122(23):2441-9; discussion 2450. doi: 10.1161/CIRCULATIONAHA.110.954446. Circulation. 2010. PMID: 21135372 Free PMC article. Review.
References
-
- Geisterfer-Lowrance AA, Kass S, Tanigawa G, Vosberg HP, McKenna W, Seidman CE, Seidman JG. A molecular basis for familial hypertrophic cardiomyopathy: a beta cardiac myosin heavy chain gene missense mutation. Cell. 1990;62:999–1006. - PubMed
-
- Watkins H, MacRae C, Thierfelder L, Chou YH, Frenneaux M, McKenna W, Seidman JG, Seidman CE. A disease locus for familial hypertrophic cardiomyopathy maps to chromosome 1q3. Nat Genet. 1993;3:333–337. - PubMed
-
- Morita H, Larson MG, Barr SC, Vasan RS, O’Donnell CJ, Hirschhorn JN, Levy D, Corey D, Seidman CE, Seidman JG, Benjamin EJ. Single-gene mutations and increased left ventricular wall thickness in the community: the Framingham Heart Study. Circulation. 2006;113:2697–2705. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
