

HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study
- PMID: 21135382
- PMCID: PMC2995535
- DOI: 10.1212/WNL.0b013e318200d727
HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study
Abstract
Objectives: This is a cross-sectional, observational study to determine the frequency and associated features of HIV-associated neurocognitive disorders (HAND) in a large, diverse sample of infected individuals in the era of combination antiretroviral therapy (CART).
Methods: A total of 1,555 HIV-infected adults were recruited from 6 university clinics across the United States, with minimal exclusions. We used standardized neuromedical, psychiatric, and neuropsychological (NP) examinations, and recently published criteria for diagnosing HAND and classifying 3 levels of comorbidity (minimal to severe non-HIV risks for NP impairment).
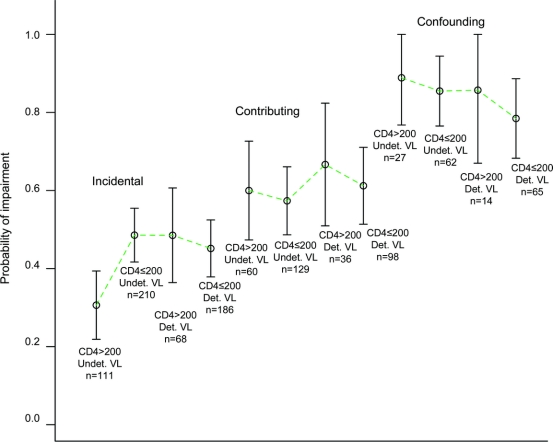
Results: Fifty-two percent of the total sample had NP impairment, with higher rates in groups with greater comorbidity burden (40%, 59%, and 83%). Prevalence estimates for specific HAND diagnoses (excluding severely confounded cases) were 33% for asymptomatic neurocognitive impairment, 12% for mild neurocognitive disorder, and only 2% for HIV-associated dementia (HAD). Among participants with minimal comorbidities (n = 843), history of low nadir CD4 was a strong predictor of impairment, and the lowest impairment rate on CART occurred in the subset with suppressed plasma viral loads and nadir CD4 ≥200 cells/mm(3) (30% vs 47% in remaining subgroups).
Conclusions: The most severe HAND diagnosis (HAD) was rare, but milder forms of impairment remained common, even among those receiving CART who had minimal comorbidities. Future studies should clarify whether early disease events (e.g., profound CD4 decline) may trigger chronic CNS changes, and whether early CART prevents or reverses these changes.
Figures
Comment in
-
The persistence of HIV-associated neurocognitive dysfunction and the effects of comorbidities.Neurology. 2010 Dec 7;75(23):2052-3. doi: 10.1212/WNL.0b013e318200d833. Neurology. 2010. PMID: 21135377 No abstract available.
References
-
- Giancola ML, Lorenzini P, Balestra P, et al. Neuroactive antiretroviral drugs do not influence neurocognitive performance in less advanced HIV-infected patients responding to highly active antiretroviral therapy. J Acquir Immune Defic Syndr 2006;41:332–337. - PubMed
-
- Sevigny JJ, Albert SM, McDermott MP, et al. An evaluation of neurocognitive status and markers of immune activation as predictors of time to death in advanced HIV infection. Arch Neurol 2007;64:97–102. - PubMed
-
- Tozzi V, Balestra P, Bellagamba R, et al. Persistence of neuropsychologic deficits despite long-term highly active antiretroviral therapy in patients with HIV-related neurocognitive impairment: prevalence and risk factors. J Acquir Immune Defic Syndr 2007;45:174–182. - PubMed
-
- Woods SP, Rippeth JD, Frol AB, et al. Interrater reliability of clinical ratings and neurocognitive diagnoses in HIV. J Clin Exp Neuropsychol 2004;26:759–778. - PubMed
Publication types
MeSH terms
Grants and funding
- K23MH079718/MH/NIMH NIH HHS/United States
- R01 AI47033/AI/NIAID NIH HHS/United States
- P01 AI 057005/AI/NIAID NIH HHS/United States
- P50DA26306/DA/NIDA NIH HHS/United States
- MH083552-02/MH/NIMH NIH HHS/United States
- R01 MH58076/MH/NIMH NIH HHS/United States
- R21 3857-53187/PHS HHS/United States
- DA026146/DA/NIDA NIH HHS/United States
- R01 MH60720/MH/NIMH NIH HHS/United States
- R01 HL84229/HL/NHLBI NIH HHS/United States
- R01MH085608/MH/NIMH NIH HHS/United States
- R01 HL95089/HL/NHLBI NIH HHS/United States
- R01 MH83552/MH/NIMH NIH HHS/United States
- U01 AG10483/AG/NIA NIH HHS/United States
- R01 DA21115/DA/NIDA NIH HHS/United States
- U13 MH81676/MH/NIMH NIH HHS/United States
- P30 MH62512/MH/NIMH NIH HHS/United States
- R01 MH78737/MH/NIMH NIH HHS/United States
- R24 MH59724/MH/NIMH NIH HHS/United States
- MH22005/MH/NIMH NIH HHS/United States
- R01 MH79881/MH/NIMH NIH HHS/United States
- MH058076/MH/NIMH NIH HHS/United States
- MH083506-02/MH/NIMH NIH HHS/United States
- P50 DA26306/DA/NIDA NIH HHS/United States
- MH085608-01/MH/NIMH NIH HHS/United States
- U01 MH083506/MH/NIMH NIH HHS/United States
- AI 069434/AI/NIAID NIH HHS/United States
- R01 MH079752/MH/NIMH NIH HHS/United States
- N01 MH22005-08/MH/NIMH NIH HHS/United States
- UO1AI69495/AI/NIAID NIH HHS/United States
- U19 AG010483/AG/NIA NIH HHS/United States
- P01 DA026146/DA/NIDA NIH HHS/United States
- R01 MH73433/MH/NIMH NIH HHS/United States
- U24 RR021992/RR/NCRR NIH HHS/United States
- R01-NS-41198/NS/NINDS NIH HHS/United States
- R01 MH79752/MH/NIMH NIH HHS/United States
- R01 MH73419/MH/NIMH NIH HHS/United States
- R21 MH083573/MH/NIMH NIH HHS/United States
- DA012065-10/DA/NIDA NIH HHS/United States
- R01 NS36524/NS/NINDS NIH HHS/United States
- R32AA17321/AA/NIAAA NIH HHS/United States
- R01 MH78748/MH/NIMH NIH HHS/United States
- AI068543/AI/NIAID NIH HHS/United States
- DA026306-01/DA/NIDA NIH HHS/United States
- R01 AI087145/AI/NIAID NIH HHS/United States
- N01MH22005/MH/NIMH NIH HHS/United States
- P01DA12065/DA/NIDA NIH HHS/United States
- K30 RR22681/RR/NCRR NIH HHS/United States
- U24 RR21382/RR/NCRR NIH HHS/United States
- U01 AI69432/AI/NIAID NIH HHS/United States
- U01 AI74521/AI/NIAID NIH HHS/United States
- R01 NS44807/NS/NINDS NIH HHS/United States
- N01MH022005/MH/NIMH NIH HHS/United States
- R01 MH067831/MH/NIMH NIH HHS/United States
- R01MH73419/MH/NIMH NIH HHS/United States
- UO1 NS32228/NS/NINDS NIH HHS/United States
- U01MH083501/MH/NIMH NIH HHS/United States
- U24 RR019701/RR/NCRR NIH HHS/United States
- RC2DA29475/DA/NIDA NIH HHS/United States
- R01MH64907/MH/NIMH NIH HHS/United States
- R32 MH77487/MH/NIMH NIH HHS/United States
- R01MH079886/MH/NIMH NIH HHS/United States
- R01 MH058076-12/MH/NIMH NIH HHS/United States
- R01 NS051132/NS/NINDS NIH HHS/United States
- U01 MH83506/MH/NIMH NIH HHS/United States
- R01 AG031224/AG/NIA NIH HHS/United States
- RC1NS068904/NS/NINDS NIH HHS/United States
- R03DA022137/DA/NIDA NIH HHS/United States
- R21 MH78728/MH/NIMH NIH HHS/United States
- R01AA13419/AA/NIAAA NIH HHS/United States
- U01MH83506/MH/NIMH NIH HHS/United States
- AI069438/AI/NIAID NIH HHS/United States
- P50DA026306/DA/NIDA NIH HHS/United States
- R01 MH075673/MH/NIMH NIH HHS/United States
- N01 MH22005/MH/NIMH NIH HHS/United States
- NIMH 22005/PHS HHS/United States
- P30 MH062512/MH/NIMH NIH HHS/United States
- P01 DA12065/DA/NIDA NIH HHS/United States
- R01 MH81861/MH/NIMH NIH HHS/United States
- U01MH083507/MH/NIMH NIH HHS/United States
- R21 MH85610/MH/NIMH NIH HHS/United States
- R01 MH61146/MH/NIMH NIH HHS/United States
- U2G PS00623/PS/NCHHSTP CDC HHS/United States
- R21 NS069355/NS/NINDS NIH HHS/United States
- AI069918/AI/NIAID NIH HHS/United States
- P30MH62512/MH/NIMH NIH HHS/United States
- R01 AG024506/AG/NIA NIH HHS/United States
- R01 MH083552/MH/NIMH NIH HHS/United States
- R01MH73433/MH/NIMH NIH HHS/United States
- R01 AG022381/AG/NIA NIH HHS/United States
- R01 AG15301/AG/NIA NIH HHS/United States
- 1R01 NS/AI34235/AI/NIAID NIH HHS/United States
- R01NS49465/NS/NINDS NIH HHS/United States
- P30 MH062512-09/MH/NIMH NIH HHS/United States
- 00-AI-0005/AI/NIAID NIH HHS/United States
- R01MH38552/MH/NIMH NIH HHS/United States
- R01 MH084796/MH/NIMH NIH HHS/United States
- AI27757/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous