

Predicting spontaneous clearance of acute hepatitis C virus in a large cohort of HIV-1-infected men
- PMID: 21139063
- PMCID: PMC3095479
- DOI: 10.1136/gut.2010.217166
Predicting spontaneous clearance of acute hepatitis C virus in a large cohort of HIV-1-infected men
Abstract
Objective: An epidemic of acute hepatitis C virus (HCV) infection in HIV-positive men-who-have-sex-with-men (MSM) is emerging in Europe, Australia and the USA. The aim of this study was to characterise the natural history of primary HCV in this setting and to assess host and viral factors which predict spontaneous clearance.
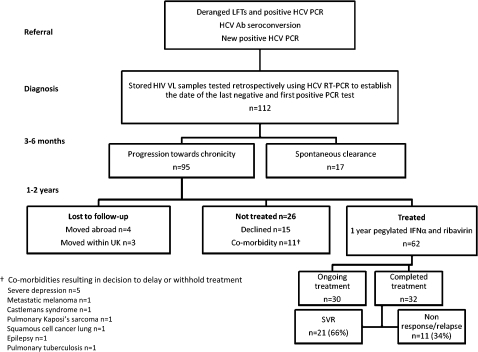
Methods: This prospective longitudinal cohort study was carried out in 112 HIV-positive patients who were followed in a single centre (the St Mary's Acute HCV Cohort). Plasma and peripheral blood mononuclear cells (PBMCs) were obtained at monthly intervals for 3 months and at 3-monthly intervals thereafter for a median of 45 months (IQR = 29-69 months). The primary end point was spontaneous clearance of HCV. Cox regression was used to assess the impact of clinical and virological variables on outcome, including liver function, CD4 count, rate of HCV RNA decline, T cell response and clonal sequence evolution within the HCV E2 envelope gene.
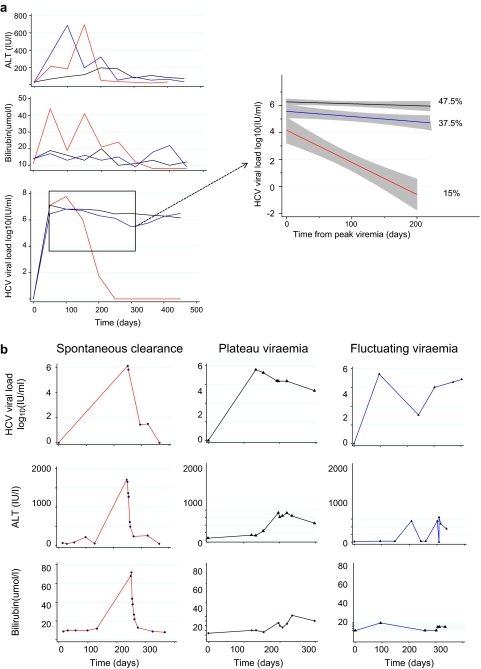
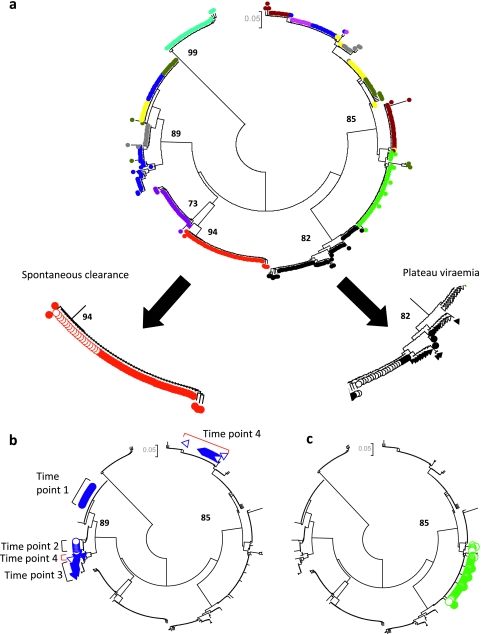
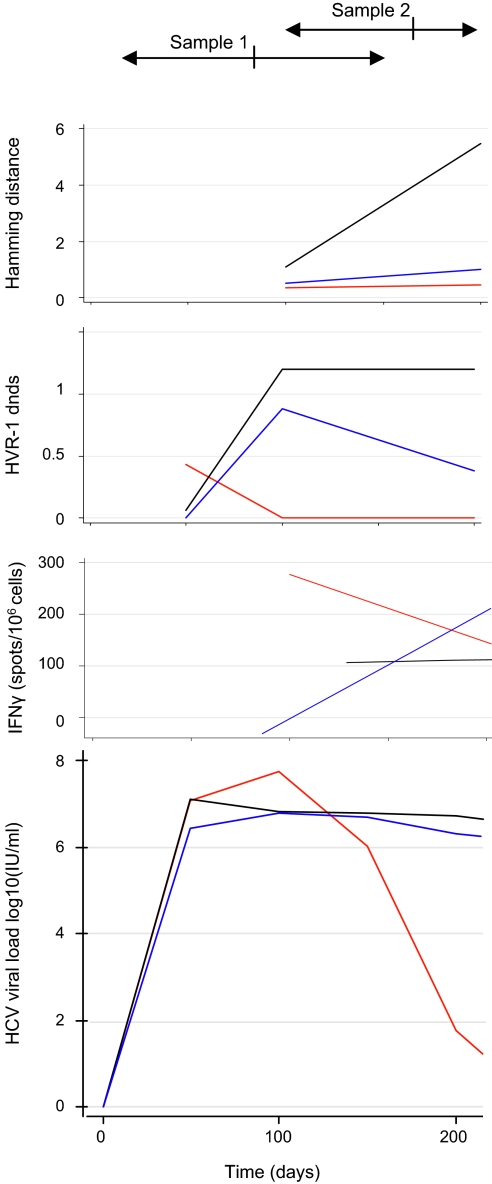
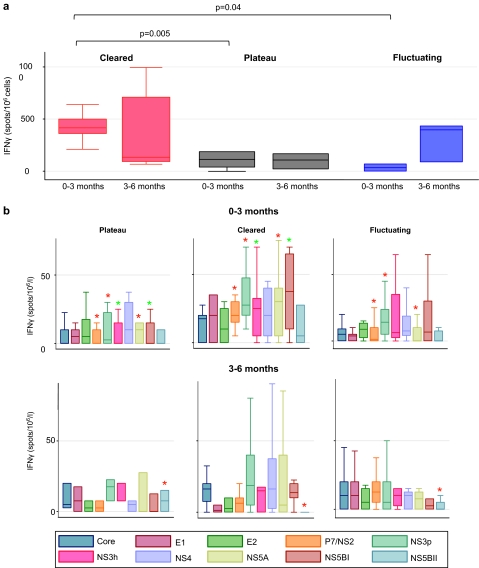
Results: 15% of patients cleared HCV spontaneously, while 85% progressed towards chronicity. The latter group included a significant proportion of 'fluctuating' progressors (37.5%), in whom a fall followed by a rise (>1 log₁₀) in viraemia was observed. This was associated with superinfection with new HCV strains and partially effective T cell responses. Spontaneous clearance was strongly associated with a 2.2 log₁₀ viral load drop within 100 days of infection (HR = 1.78; p < 0.0001), elevated bilirubin (≥ 40 μmol/l; HR = 5.04; p = 0.006), elevated alanine aminotransferase (ALT; ≥ 1000 IU/ml; HR = 2.62; p = 0.048) and baseline CD4 count ≥ 650 × 10⁶/l (HR = 2.66; p = 0.045), and only occurred in patients with genotype 1 infection. Evolution to spontaneous clearance occurred in patients with low viral diversity in the presence of an early multispecific T cell response.
Conclusions: Spontaneous clearance of acute HCV in HIV-positive men can be predicted by a rapid decline in viral load, high CD4 count, elevated bilirubin and ALT, and is associated with low viral diversity and strong T cell responses.
Conflict of interest statement
Figures
References
-
- Choo QL, Kuo G, Weiner AJ, et al. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science 1989;244:359–62 - PubMed
-
- Wiese M, Grungreiff K, Guthoff W, et al. Outcome in a hepatitis C (genotype 1b) single source outbreak in Germany—a 25-year multicenter study. J Hepatol 2005;43:590–8 - PubMed
-
- Martinez-Bauer E, Forns X, Armelles M, et al. Hospital admission is a relevant source of hepatitis C virus acquisition in Spain. J Hepatol 2008;48:20–7 - PubMed
-
- Santantonio T, Medda E, Ferrari C, et al. Risk factors and outcome among a large patient cohort with community-acquired acute hepatitis C in Italy. Clin Infect Dis 2006;43:1154–9 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials