

Moving the tipping point: the decision to anticoagulate patients with atrial fibrillation
- PMID: 21139092
- PMCID: PMC3058150
- DOI: 10.1161/CIRCOUTCOMES.110.958108
Moving the tipping point: the decision to anticoagulate patients with atrial fibrillation
Abstract
Background: The rate of ischemic stroke associated with traditional risk factors for patients with atrial fibrillation has declined over the past 2 decades. Furthermore, new and potentially safer anticoagulants are on the horizon. Thus, the balance between risk factors for stroke and benefit of anticoagulation may be shifting.
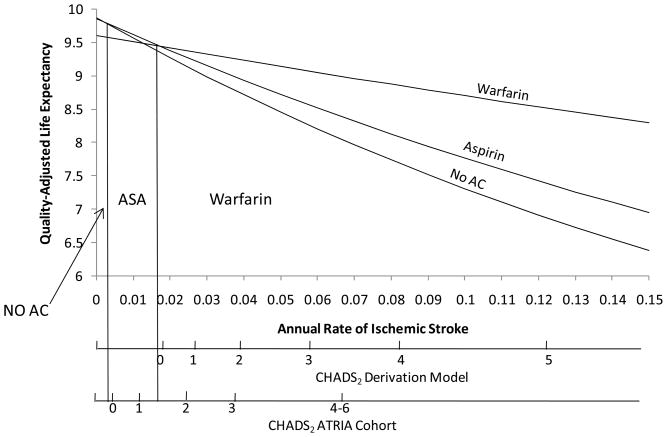
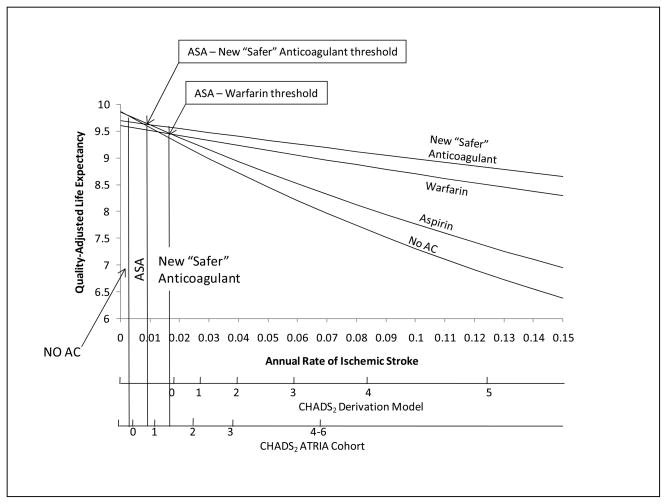
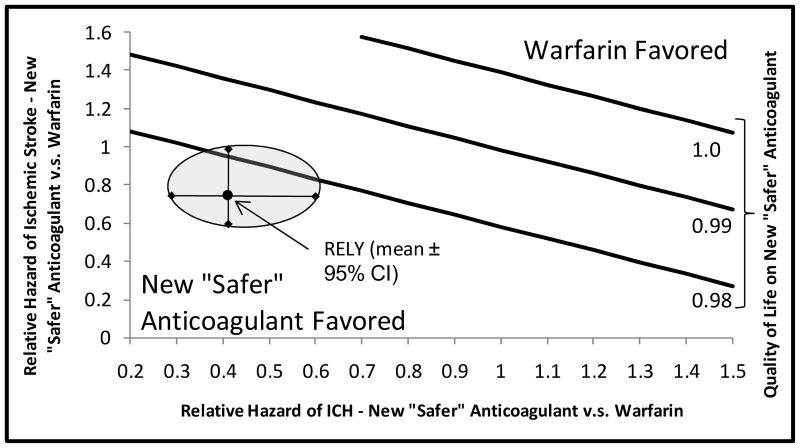
Methods and results: The Markov state transition decision model was used to analyze the CHADS(2) score, above which anticoagulation is preferred, first using the stroke rate predicted for the CHADS(2) derivation cohort, and then using the stroke rate from the more contemporary AnTicoagulation and Risk Factors In Atrial Fibrillation cohort for any CHADS(2) score. The base case was a 69-year-old man with atrial fibrillation. Interventions included oral anticoagulant therapy with warfarin or a hypothetical "new and safer" anticoagulant (based on dabigatran), no antithrombotic therapy, or aspirin. Warfarin is preferred above a stroke rate of 1.7% per year, whereas aspirin is preferred at lower rates of stroke. Anticoagulation with warfarin is preferred even for a score of 0 using the higher rates of the older CHADS(2) derivation cohort. Using more contemporary and lower estimates of stroke risk raises the threshold for use of warfarin to a CHADS(2) score ≥2. However, anticoagulation with a "new, safer" agent, modeled on the results of the Randomized Evaluation of Long-Term Anticoagulation Therapy trial of dabigatran, leads to a lowering of the threshold for anticoagulation to a stroke rate of 0.9% per year.
Conclusions: Use of a more contemporary estimate of stroke risk shifts the "tipping point," such that anticoagulation is preferred at a higher CHADS(2) score, reducing the number of patients for whom anticoagulation is recommended. The introduction of "new, safer" agents, however, would shift the tipping point in the opposite direction.
Figures
Comment in
-
Quality of stroke prevention care in atrial fibrillation: many moving targets.Circ Cardiovasc Qual Outcomes. 2011 Jan 1;4(1):5-8. doi: 10.1161/CIRCOUTCOMES.110.959890. Circ Cardiovasc Qual Outcomes. 2011. PMID: 21245458 No abstract available.
References
-
- Flaherty ML, Kissela B, Woo D, Kleindorfer D, Alwell K, Sekar P, Moomaw CJ, Haverbusch M, Broderick JP. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology. 2007;68:116–121. - PubMed
-
- Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med. 2004;164:880–884. - PubMed
-
- Lakshminarayan K, Solid CA, Collins AJ, Anderson DC, Herzog CA. Atrial fibrillation and stroke in the general medicare population: a 10-year perspective (1992 to 2002) Stroke. 2006;37:1969–1974. - PubMed
-
- Arima H, Hart RG, Colman S, Chalmers J, Anderson C, Rodgers A, Woodward M, MacMahon S, Neal B. Perindopril-based blood pressure-lowering reduces major vascular events in patients with atrial fibrillation and prior stroke or transient ischemic attack. Stroke. 2005;36:2164–2169. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
