

Giant cell tumor of bone: Is curettage the answer?
- PMID: 21139761
- PMCID: PMC2989132
- DOI: 10.4103/0019-5413.32040
Giant cell tumor of bone: Is curettage the answer?
Abstract
Background: Giant cell tumors (GCT) are neoplasms of mesenchymal stromal cells with varied manifestations. There is no uniform accepted treatment protocol for these tumors,
Materials and methods: 49 cases of proven giant cell tumors of appendicular skeleton, 27 prospective and 22 retrospective constituteed this study. The retrospective cases were collected by using computerized data base collection method. The patients were evaluated clinically, radiologically and by histology. Companacci grading and Enneking staging was used in the study. Two treatment modalities were used a) extended curettage (with/ without bone grafting/ cementation) or b) wide excision and reconstruction with a prosthesis or arthrodesis. Functional evaluation was done by Enneking's system. Chi square tests, mann-whitney test and ANOVA were used for statistical analysis.
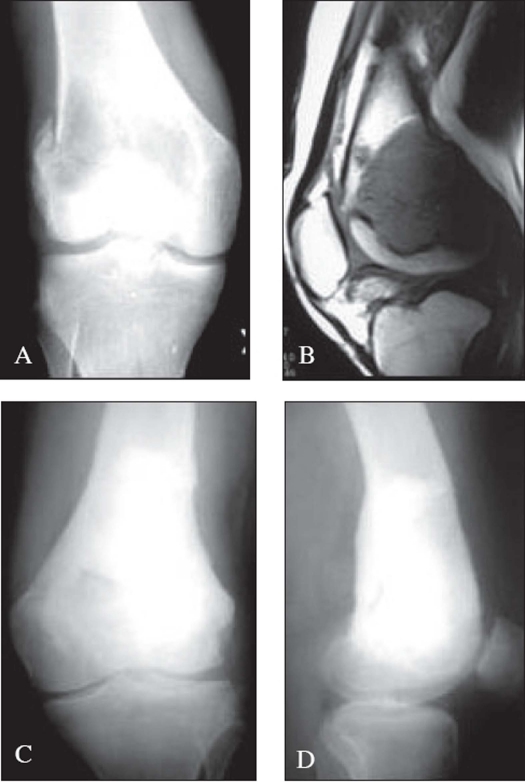
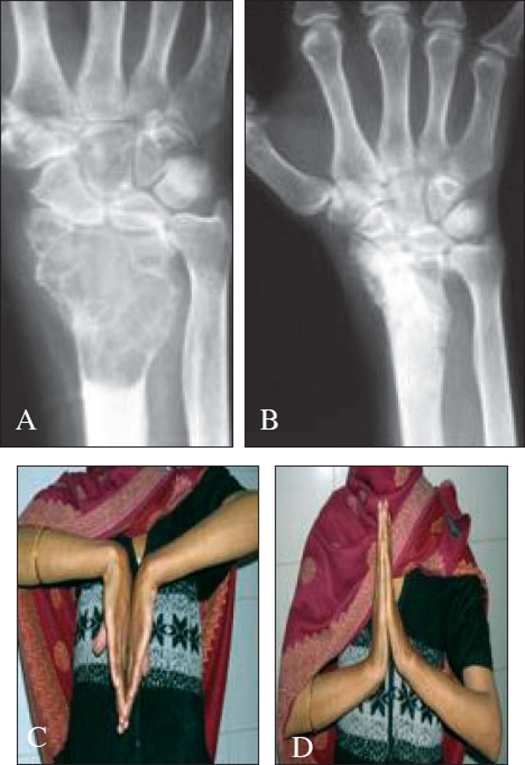
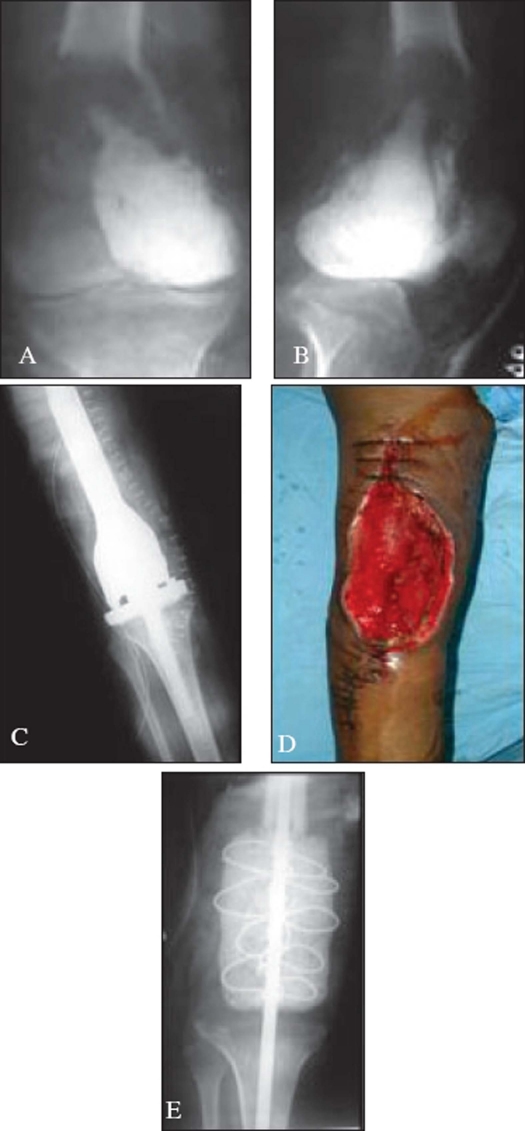
Results: The average age was 26.82 years (16-50 years). 25 patients (51%) were recurrent GCT at presentation. The commonest site was lower end of femur (16 cases, 32.65%) and upper end of tibia (13 cases, 26.53%). 40 (81.63%) tumors had less than 5 mm of subchondral bone free of tumor. 35 (71.43%) tumors were Enneking's surgical stage III and companacci grade III. Pathological fractures were seen in 12 (24.49%) cases. Intra-lesional currettage was used in 28 and enbloc excision in 19 patients and 2 (4.08%) underwent amputation. The average follow up period was 18.6 months (range 2-84). One recurrence was seen in a grade III recurrent distal radial lesion in the intralesional curettage group (3.57%) Enneking's functional score with intralesional curettage (25.41) was better than enbloc excision (21.37). Enbloc excision had higher rates of infections (36.84 % Vs 25%) and soft tissue coverage problems (21.05% Vs 0).
Conclusion: Intralesional therapy has a better functional outcome and less complications than enbloc excision, albeit with a high recurrence rate which can however be effectively treated with repeat extended curettage.
Keywords: Adjuvant therapy; extended curettage; giant cell tumor.
Conflict of interest statement
Figures
References
-
- McDonald DJ, Sim FH, McLeod RA, Dahlin DC. Giant-cell tumor of bone. J Bone Joint Surg Am. 1986;68:235–42. - PubMed
-
- Malawer MM, Bickels J, Meller I, Buch RG, Henshaw RM, Kollender Y. Cryosurgery in the treatment of giant cell tumor. A long-term followup study. Clin Orthop Relat Res. 1999;359:176–88. - PubMed
-
- Duncan CP, Morton KS, Arthur JF. Giant cell tumor of bone: Its aggressiveness and potential for malignant change. Can J Surg. 1983;26:475–6. - PubMed
-
- Komiya S, Inoue A, Nakashima M, Ueno A, Fujikawa K, Ikuta H. Prognostic factors in giant cell tumor of bone. A modified histological grading system useful as a guide to prognosis. Arch Orthop Trauma Surg. 1986;105:67–72. - PubMed
-
- Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am. 1987;69:106–14. - PubMed
LinkOut - more resources
Full Text Sources