

Role of early minimal-invasive spine fixation in acute thoracic and lumbar spine trauma
- PMID: 21139794
- PMCID: PMC2989516
- DOI: 10.4103/0019-5413.37003
Role of early minimal-invasive spine fixation in acute thoracic and lumbar spine trauma
Abstract
Polytraumatized patients following a severe trauma suffer from substantial disturbances of the immune system. Secondary organ dysfunction syndromes due to early hyperinflammation and late immunparalysis contribute to adverse outcome. Consequently the principle of damage control surgery / orthopedics developed in the last two decades to limit secondary iatrogenic insult in these patients. New percutaneous internal fixators provide implants for a damage control approach of spinal trauma in polytraumatized patients. The goal of this study is to evaluate the feasibility of minimal-invasive instrumentation in the setting of minor and major trauma and to discuss the potential benefits and drawbacks of this procedure.
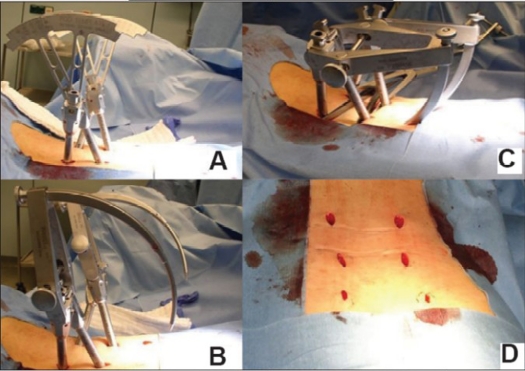
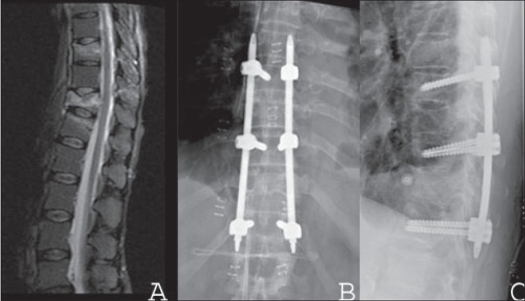
Materials and methods: The present study is a prospective analysis of 76 consecutive patients (mean age 53.3 years) with thoracolumbar spine fractures following major or minor trauma from August 2003 to January 2007 who were subjected to minimal-invasive dorsal instrumentation using CD Horizon(®) Sextant™ Rod Insertion System and Longitude™ Rod Insertion System (Medtronic(®) Sofamor Danek). Perioperative and postoperative outcome measures including e.g. local and systemic complications were assessed and discussed.
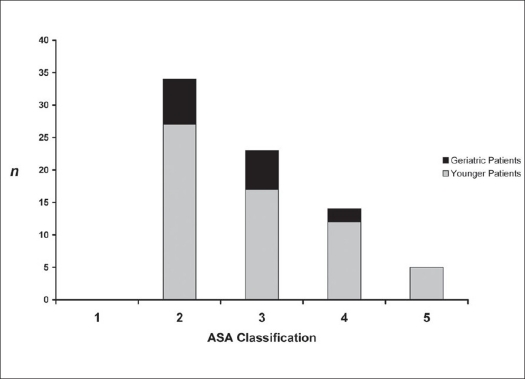
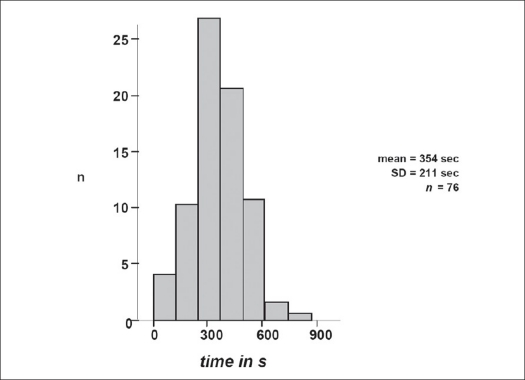
Results: Forty-nine patients (64.5%) suffered from minor trauma (Injury Severity Score <16). Polytraumatized patients (n=27; 35.5%) had associated chest (n=20) and traumatic brain injuries (n=22). For mono- and bisegmental dorsal instrumentation the Sextant™ was used in 60 patients, whereas in 16 longer ranging instrumentations the (prototype) Longitude™ system was implanted. Operation time was substantially lower than in conventional approach at minimum 22.5 min for Sextant and 36.2 min for Longitude™, respectively. Geriatric patients with high perioperative risk according to ASA classification benefited from the less invasive approach and lack of approach-related complications including no substantial blood loss.
Conclusion: Low rate of approach-related complications in association with short operation time and virtually no blood loss is beneficial in the setting of polytraumatized patients regarding damage control orthopedics, as well as in geriatric patients with high perioperative risk. The minimal-invasive instrumentation of the spine is associated with beneficial outcome in a selected patient population.
Keywords: Damage control; minimally invasive; polytrauma; spinal fracture; spinal instrumentation.
Conflict of interest statement
Figures

References
-
- Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and lumbar injuries. Eur Spine J. 1994;3:184–201. - PubMed
-
- Thomsen K, Christensen FB, Eiskjaer SP, Hansen ES, Fruensgaard S, Bünger CE. 1997 Volvo Award winner in clinical studies: The effect of pedicle screw instrumentation on functional outcome and fusion rates in posterolateral lumbar spinal fusion: A prospective, randomized clinical study. Spine. 1997;22:2813–22. - PubMed
-
- Mathews HH, BH Long. Endoscopy assisted percutaneous anterior interbody fusion with subcutaneous suprafascial internal fixation: Evolution of technique and surgical considerations. Orthopaedics. 1995;3:353–66.
-
- Ringel F, Stoffel M, Stüer C, Meyer B. Minimally invasive transmuscular pedicle screw fixation of the thoracic and lumbar spine. Neurosurgery. 2006;59:ONS361–7. - PubMed
LinkOut - more resources
Full Text Sources