

In the presence of strong P2Y12 receptor blockade, aspirin provides little additional inhibition of platelet aggregation
- PMID: 21143373
- PMCID: PMC3064407
- DOI: 10.1111/j.1538-7836.2010.04160.x
In the presence of strong P2Y12 receptor blockade, aspirin provides little additional inhibition of platelet aggregation
Abstract
Background: Aspirin and antagonists of platelet ADP P2Y(12) receptors are often coprescribed for protection against thrombotic events. However, blockade of platelet P2Y(12) receptors can inhibit thromboxane A(2) (TXA(2))-dependent pathways of platelet activation independently of aspirin.
Objectives: To assess in vitro whether aspirin adds additional antiaggregatory effects to strong P2Y(12) receptor blockade.
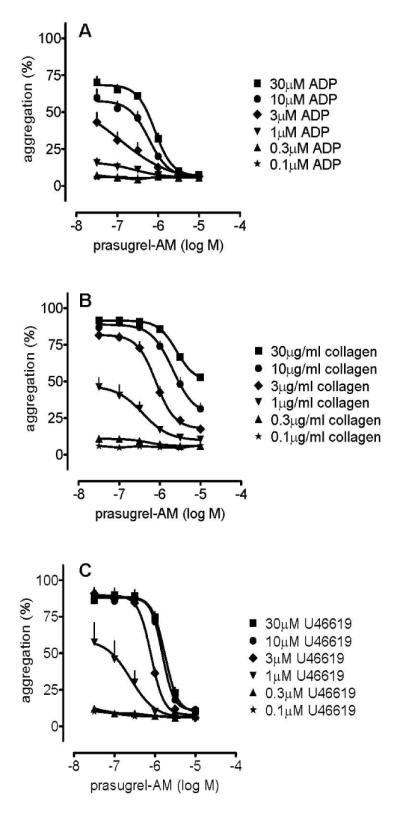
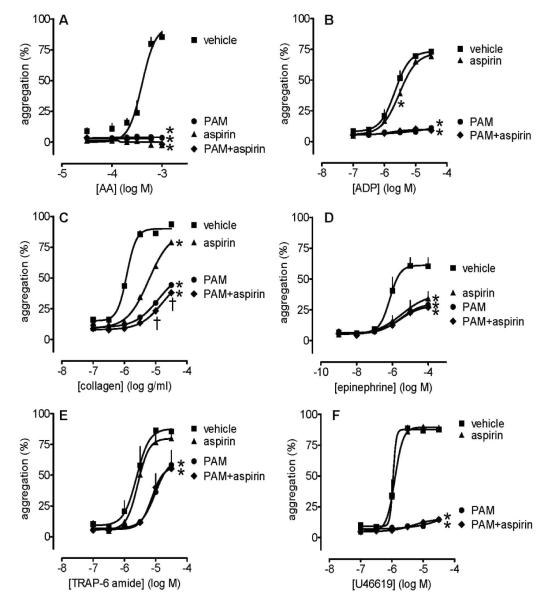
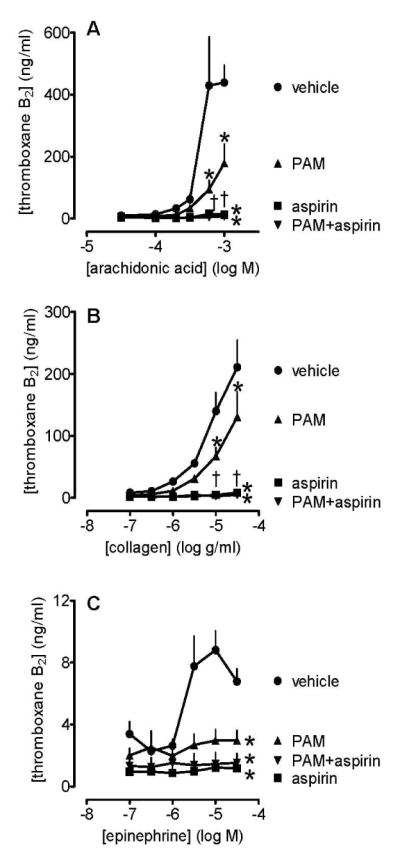
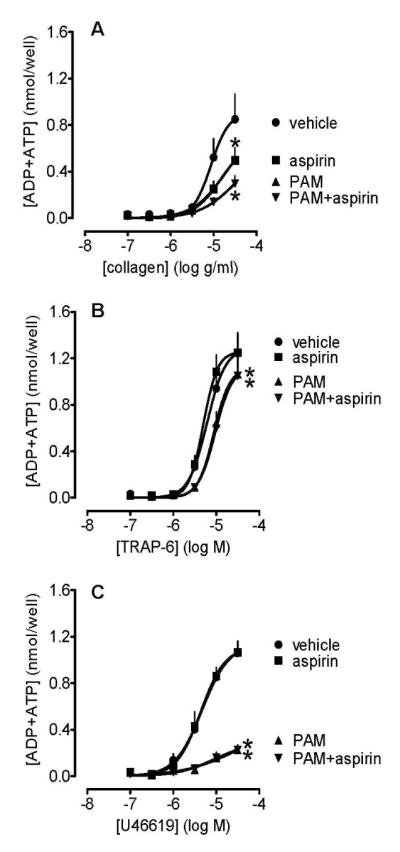
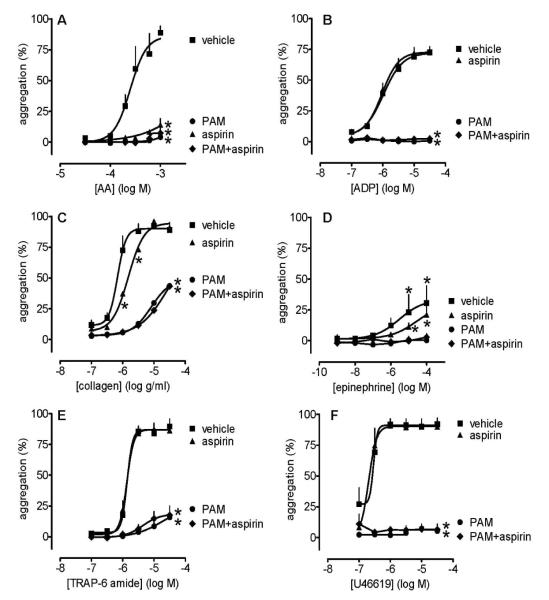
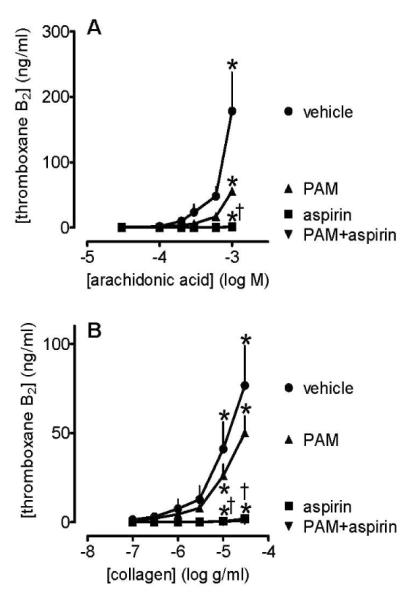
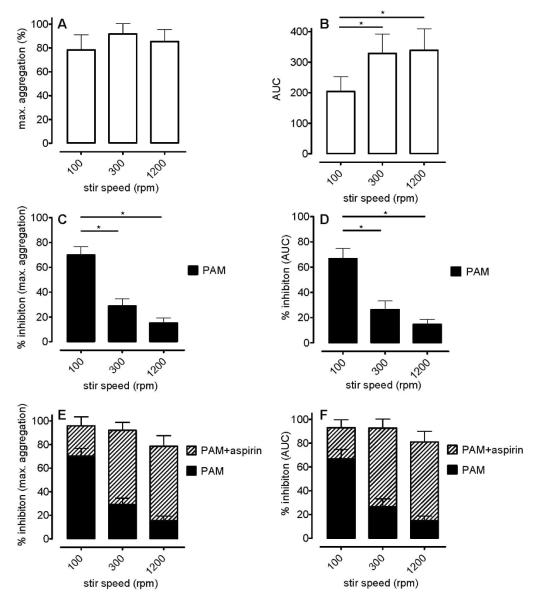
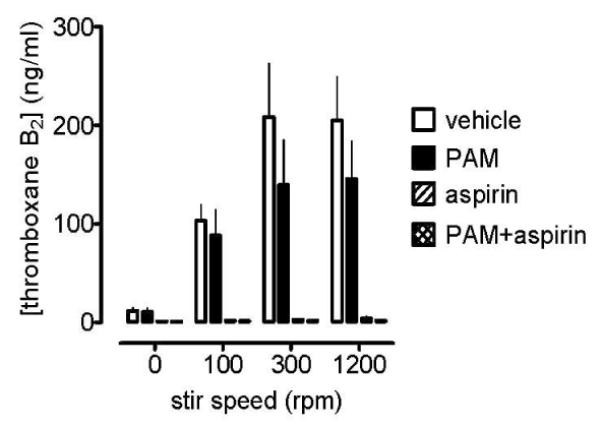
Methods: With the use of platelet-rich plasma from healthy volunteers, determinations were made in 96-well plates of platelet aggregation, TXA(2) production and ADP/ATP release caused by ADP, arachidonic acid, collagen, epinephrine, TRAP-6 amide and U46619 (six concentrations of each) in the presence of prasugrel active metabolite (PAM; 0.1-10 μmol L(-1)), aspirin (30 μmol L(-1)), PAM + aspirin or vehicle. results: PAM concentration-dependently inhibited aggregation; for example, aggregation in response to all concentrations of ADP and U46619 was inhibited by ≥ 95% by PAM at > 3 μmol L(-1) . In further tests of PAM (3 μmol L(-1)), aspirin (30 μmol L(-1)) and PAM + aspirin, aspirin generally failed to produce more inhibition than PAM or additional inhibition to that caused by PAM. The antiaggregatory effects of PAM were associated with reductions in the platelet release of both TXA(2) and ATP + ADP. Similar effects were found when either citrate or lepirudin were used as anticoagulants, and when traditional light transmission aggregometry was conducted at low stirring speeds.
Conclusions: P2Y(12) receptors are critical to the generation of irreversible aggregation through the TXA(2) -dependent pathway. As a result, strong P2Y(12) receptor blockade alone causes inhibition of platelet aggregation that is little enhanced by aspirin. The clinical relevance of these observations remains to be determined.
© 2011 International Society on Thrombosis and Haemostasis.
Figures
References
-
- Saw J, Madsen EH, Chan S, Maurer-Spurej E. The ELAPSE (Evaluation of Long-Term Clopidogrel Antiplatelet and Systemic Anti-Inflammatory Effects) Study. J Am Coll Cardiol. 2008;52:1826–33. - PubMed
-
- Mehta SR, Yusuf S, Peters RJG, Bertrand ME, Lewis BS, Natarajan MK, Malmberg K, Rupprecht H-J, Zhao F, Chrolavicius S, Copland I, Fox KAA. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001;358:527–33. - PubMed
-
- Bhatt DL. Role of antiplatelet therapy across the spectrum of patients with coronary artery disease. Am J Cardiol. 2009;103:11A–19A. - PubMed
-
- Jakubowski JA, Winters KJ, Naganuma H, Wallentin L. Prasugrel: a novel thienopyridine antiplatelet agent. A review of preclinical and clinical studies and the mechanistic basis for its distinct antiplatelet profile. Cardiovasc Drug Rev. 2007;25:357–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
