

Neonatal Procalcitonin Intervention Study (NeoPInS): Effect of Procalcitonin-guided decision making on duration of antibiotic therapy in suspected neonatal early-onset sepsis: A multi-centre randomized superiority and non-inferiority Intervention Study
- PMID: 21143869
- PMCID: PMC3016366
- DOI: 10.1186/1471-2431-10-89
Neonatal Procalcitonin Intervention Study (NeoPInS): Effect of Procalcitonin-guided decision making on duration of antibiotic therapy in suspected neonatal early-onset sepsis: A multi-centre randomized superiority and non-inferiority Intervention Study
Abstract
Background: Early diagnosis and treatment of the newborn infant with suspected sepsis are essential to prevent severe and life threatening complications. Diagnosis of neonatal sepsis is difficult because of the variable and nonspecific clinical presentation. Therefore, many newborns with nonspecific symptoms are started on antibiotic treatment before the presence of sepsis has been proven. With our recently published single-centre intervention study we were able to show that Procalcitonin determinations allowed to shorten the duration of antibiotic therapy in newborns with suspected early-onset sepsis.
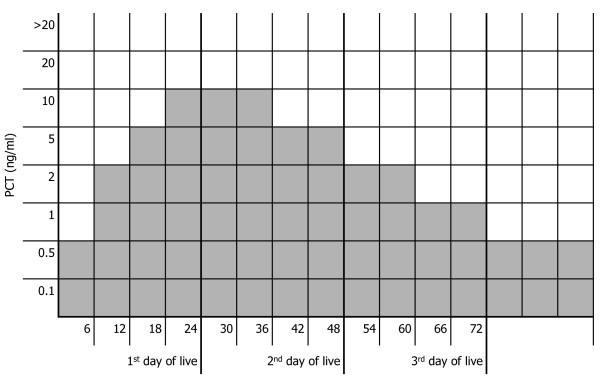
Methods/design: The study is designed as randomized controlled international multicenter intervention trial on the efficacy and safety of Procalcitonin guided treatment. Term and near-term infants (gestational age ≥ 34 0/7 weeks) with suspected sepsis in the first 3 days of life requiring empiric antibiotic therapy will be included. The duration of antibiotic therapy in the standard group is based on the attending physician's assessment of the likelihood of infection (infection unlikely, possible, probable or proven). In the Procalcitonin group, if infection is considered to be unlikely or possible, antibiotic therapy is discontinued when two consecutive Procalcitonin values are within the normal range. Co-primary outcome measures are the duration of antibiotic therapy (superiority aspect of the trial) and the proportion of infants with a recurrence of infection requiring additional courses of antibiotic therapy and/or death in the first month of life (safety of study intervention, non-inferiority aspect of the trial). The number of infants to be included equals 800 per arm. With these numbers the power of the study to demonstrate superiority for duration of antibiotic therapy as well as non-inferiority regarding safety, i.e. excluding a disadvantage difference larger than 2% for the experimental arm, will both be greater than 80%.
Discussion: Benefit of the study is a possible limitation of unnecessary use of antibiotics. The results of our first study suggest that there is a low risk on discontinuing antibiotic treatment too early, resulting in the development of a neonatal infection with its morbidity and mortality.
Trial registration: This trial is registered in the U.S. National Institutes of Health's register, located at http://www.clinicaltrials.gov. (NCT00854932).
Figures
References
-
- Afroza S. Neonatal Sepsis - a global problem: an overview. Mymensingh Med J. 2006;15:108–114. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
