

A comparative study on the efficacy of 10% hypertonic saline and equal volume of 20% mannitol in the treatment of experimentally induced cerebral edema in adult rats
- PMID: 21143951
- PMCID: PMC3004923
- DOI: 10.1186/1471-2202-11-153
A comparative study on the efficacy of 10% hypertonic saline and equal volume of 20% mannitol in the treatment of experimentally induced cerebral edema in adult rats
Abstract
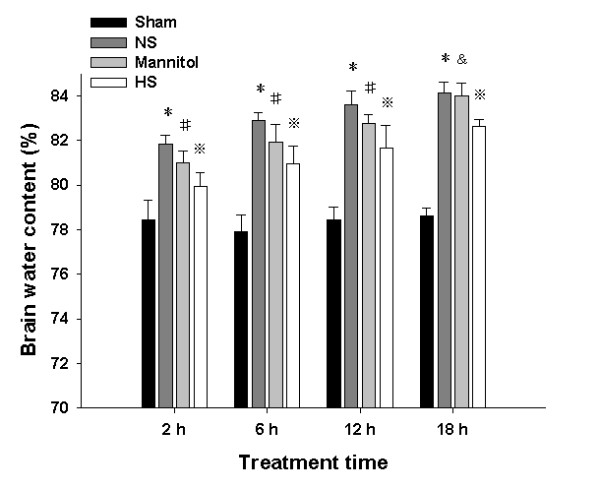
Background: Hypertonic saline and mannitol are commonly used in the treatment of cerebral edema and elevated intracranial pressure (ICP) at present. In this connection, 10% hypertonic saline (HS) alleviates cerebral edema more effectively than the equal volume of 20% mannitol. However, the exact underlying mechanism for this remains obscure. This study aimed to explore the possible mechanism whereby 10% hypertonic saline can ameliorate cerebral edema more effectively than mannitol.
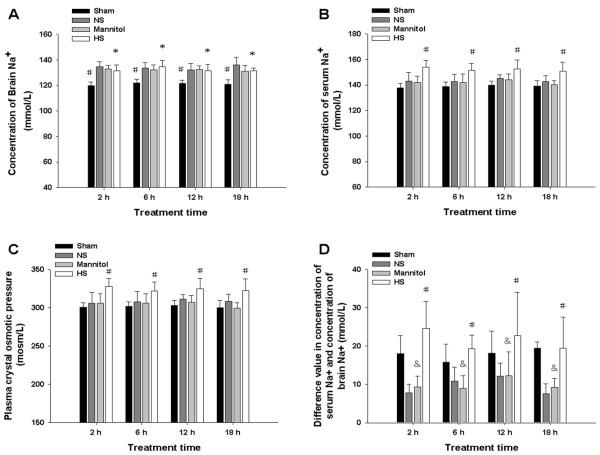
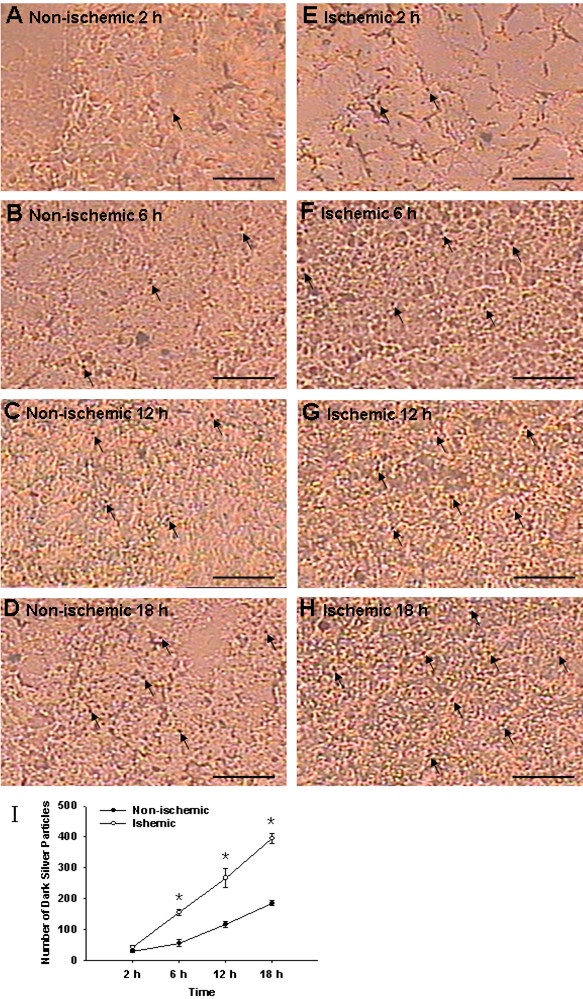
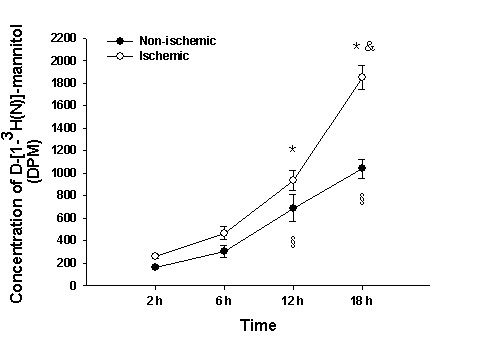
Results: Adult male Sprague-Dawley (SD) rats were subjected to permanent right-sided middle cerebral artery occlusion (MCAO) and treated with a continuous intravenous infusion of 10% HS, 20% mannitol or D-[1-3H(N)]-mannitol. Brain water content (BWC) as analyzed by wet-to-dry ratios in the ischemic hemisphere of SD rats decreased more significantly after 10% HS treatment compared with 20% mannitol. Concentration of serum Na+ and plasma crystal osmotic pressure of the 10% HS group at 2, 6, 12 and 18 h following permanent MCAO increased significantly when compared with 20% mannitol treated group. Moreover, there was negative correlation between the BWC of the ipsilateral ischemic hemisphere and concentration of serum Na+, plasma crystal osmotic pressure and difference value of concentration of serum Na+ and concentration of brain Na+ in ipsilateral ischemic hemisphere in the 10% HS group at the various time points after MCAO. A remarkable finding was the progressive accumulation of mannitol in the ischemic brain tissue.
Conclusions: We conclude that 10% HS is more effective in alleviating cerebral edema than the equal volume of 20% mannitol. This is because 10% HS contributes to establish a higher osmotic gradient across BBB and, furthermore, the progressive accumulation of mannitol in the ischemic brain tissue counteracts its therapeutic efficacy on cerebral edema.
Figures
References
-
- Boulard G, Marguinaud E, Sesay M. Osmotic cerebral oedema: the role of plasma osmolarity and blood brain barrier. Ann Fr Anesth Reanim. 2003;22:215–9. - PubMed
-
- Pérez-Pérez AJ, Pazos B, Sobrado J, Gonzalez L, Gándara A. Acute renal failure following massive mannitol infusion. Am J Nephrol. 2002;22:573–575. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
