

Pulmonary pathways and mechanisms regulating transpulmonary shunting into the general circulation: an update
- PMID: 21144922
- PMCID: PMC4385739
- DOI: 10.1016/S0020-1383(10)70004-8
Pulmonary pathways and mechanisms regulating transpulmonary shunting into the general circulation: an update
Abstract
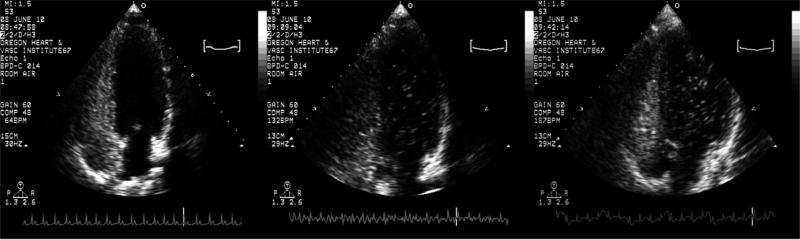
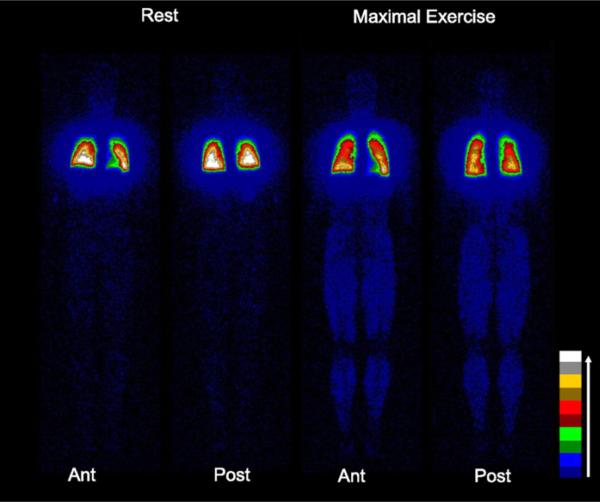
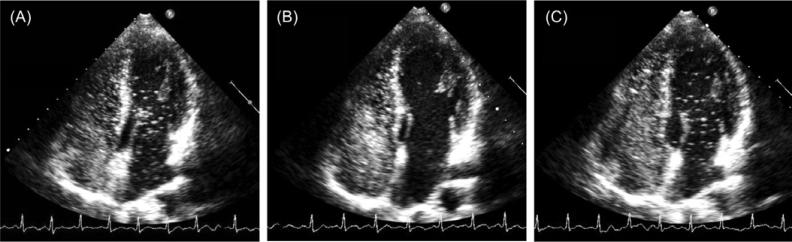
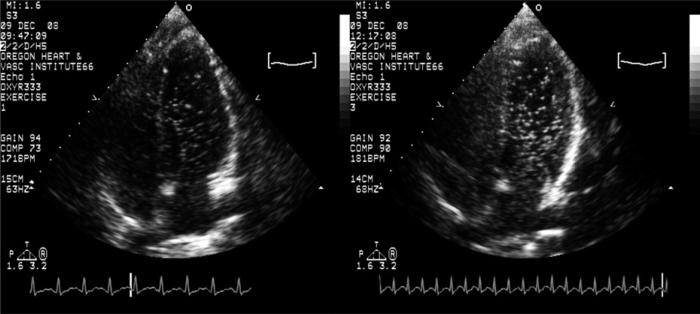
Embolic insults account for a significant number of neurologic sequelae following many routine surgical procedures. Clearly, these post-intervention embolic events are a serious public health issue as they are potentially life altering. However, the pathway these emboli utilize to bypass the pulmonary microcirculatory sieve in patients without an intracardiac shunt such as an atrial septal defect or patent foramen ovale, remains unclear. In the absence of intracardiac routes and large diameter pulmonary arteriovenous malformations, inducible large diameter intrapulmonary arteriovenous anastomoses in otherwise healthy adult humans may prove to be the best explanation. Our group and others have demonstrated that inducible large diameter intrapulmonary arteriovenous anastomoses are closed at rest but can open during hyperdynamic conditions such as exercise in more than 90% of healthy humans. Furthermore, the patency of these intrapulmonary anastomoses can be modulated through the fraction of inspired oxygen and by body positioning. Of particular clinical interest, there appears to be a strong association between arterial hypoxemia and neurologic insults, suggesting a breach in the filtering ability of the pulmonary microvasculature under these conditions. In this review, we present evidence demonstrating the existence of inducible intrapulmonary arteriovenous anastomoses in healthy humans that are modulated by exercise, oxygen tension and body positioning. Additionally, we identify several clinical conditions associated with both arterial hypoxemia and an increased risk for embolic insults. Finally, we suggest some precautionary measures that should be taken during interventions to keep intrapulmonary arteriovenous anastomoses closed in order to prevent or reduce the incidence of paradoxical embolism.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures
References
-
- Basnyat B, Wu T, Gertsch JH. Neurological conditions at altitude that fall outside the usual definition of altitude sickness. High Alt Med Biol. 2004;5:171–9. - PubMed
-
- Burkard ME, Van Liew HD. Simulation of exchanges of multiple gases in bubbles in the body. Respir Physiol. 1994;95:131–45. - PubMed
-
- Butler BD, Hills BA. The lung as a filter for microbubbles. J Appl Physiol. 1979;47:537–43. - PubMed
-
- Cheney FW, Pavlin J, Ferens J, Allen D. Effect of pulmonary microembolism on arteriovenous shunt flow. J ThoracCardiovascSurg. 1978;76:473–78. - PubMed
-
- Danesh J, Collins R, Appleby P, Peto R. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: meta-analyses of prospective studies. JAMA. 1998;279:1477–82. - PubMed
