

Predictive markers for AD in a multi-modality framework: an analysis of MCI progression in the ADNI population
- PMID: 21146621
- PMCID: PMC3035743
- DOI: 10.1016/j.neuroimage.2010.10.081
Predictive markers for AD in a multi-modality framework: an analysis of MCI progression in the ADNI population
Abstract
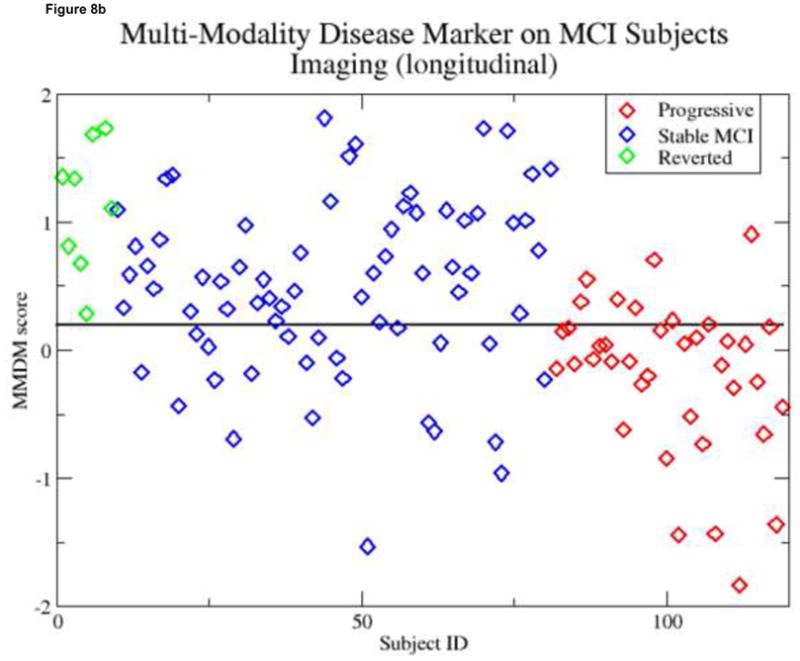
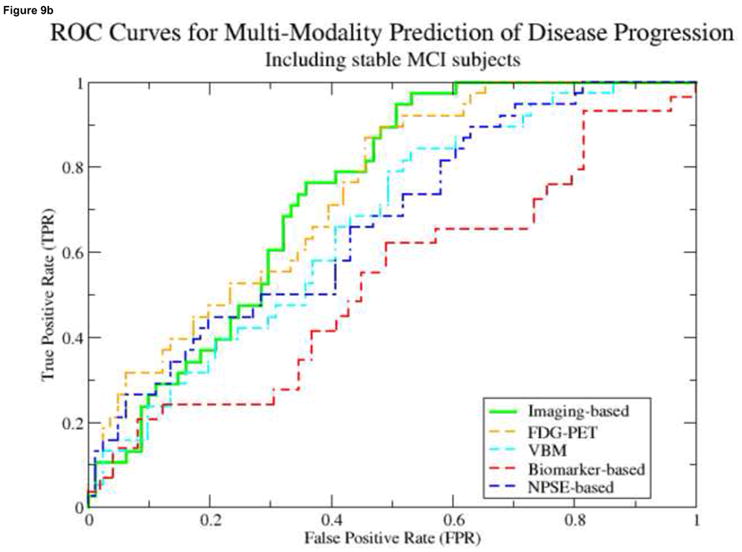
Alzheimer's Disease (AD) and other neurodegenerative diseases affect over 20 million people worldwide, and this number is projected to significantly increase in the coming decades. Proposed imaging-based markers have shown steadily improving levels of sensitivity/specificity in classifying individual subjects as AD or normal. Several of these efforts have utilized statistical machine learning techniques, using brain images as input, as means of deriving such AD-related markers. A common characteristic of this line of research is a focus on either (1) using a single imaging modality for classification, or (2) incorporating several modalities, but reporting separate results for each. One strategy to improve on the success of these methods is to leverage all available imaging modalities together in a single automated learning framework. The rationale is that some subjects may show signs of pathology in one modality but not in another-by combining all available images a clearer view of the progression of disease pathology will emerge. Our method is based on the Multi-Kernel Learning (MKL) framework, which allows the inclusion of an arbitrary number of views of the data in a maximum margin, kernel learning framework. The principal innovation behind MKL is that it learns an optimal combination of kernel (similarity) matrices while simultaneously training a classifier. In classification experiments MKL outperformed an SVM trained on all available features by 3%-4%. We are especially interested in whether such markers are capable of identifying early signs of the disease. To address this question, we have examined whether our multi-modal disease marker (MMDM) can predict conversion from Mild Cognitive Impairment (MCI) to AD. Our experiments reveal that this measure shows significant group differences between MCI subjects who progressed to AD, and those who remained stable for 3 years. These differences were most significant in MMDMs based on imaging data. We also discuss the relationship between our MMDM and an individual's conversion from MCI to AD.
Copyright © 2010 Elsevier Inc. All rights reserved.
Figures























References
-
- Albert MS, Moss MB, Tanzi R, Jones K. Preclinical prediction of AD using neuropsychological tests. Journal of the International Neuropsychological Society. 2001;7(05):631–639. - PubMed
-
- Arimura H, Yoshiura T, Kumazawa S, Tanaka K, Koga H, Mihara F, Honda H, Sakai S, Toyofuku F, Higashida Y. Automated method for identification of patients with Alzheimer’s disease based on three-dimensional MR images. Academic Radiology. 2008;15(3):274–284. - PubMed
-
- Ashburner J. A fast diffeomorphic image registration algorithm. Neuroimage. 2007;38(1):95–113. - PubMed
-
- Ashburner J, Friston KJ. Voxel-Based Morphometry - The Methods. Neuroimage. 2000;11(6):805–821. - PubMed
-
- Bakir G, Hofmann T, Schölkopf B. Predicting structured data. The MIT Press; 2007.
Publication types
MeSH terms
Substances
Grants and funding
- K01 AG030514/AG/NIA NIH HHS/United States
- P30 HD003352/HD/NICHD NIH HHS/United States
- R21-AG034315/AG/NIA NIH HHS/United States
- R21 AG034315/AG/NIA NIH HHS/United States
- 5T15LM007359/LM/NLM NIH HHS/United States
- T15 LM007359/LM/NLM NIH HHS/United States
- 1UL1RR025011/RR/NCRR NIH HHS/United States
- P30 AG010129/AG/NIA NIH HHS/United States
- R01-AG021155/AG/NIA NIH HHS/United States
- P50 AG033514/AG/NIA NIH HHS/United States
- U01 AG024904/AG/NIA NIH HHS/United States
- U19 AG010483/AG/NIA NIH HHS/United States
- UL1 RR025011/RR/NCRR NIH HHS/United States
- R01 AG021155/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
