

Intraductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment
- PMID: 21147870
- PMCID: PMC3227924
- DOI: 10.1634/theoncologist.2010-0151
Intraductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment
Abstract
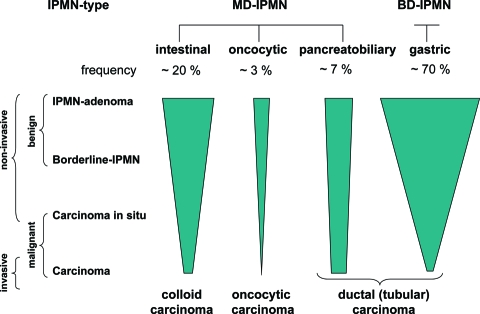
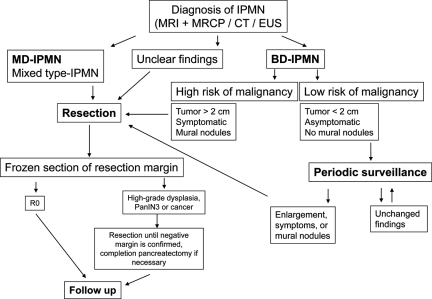
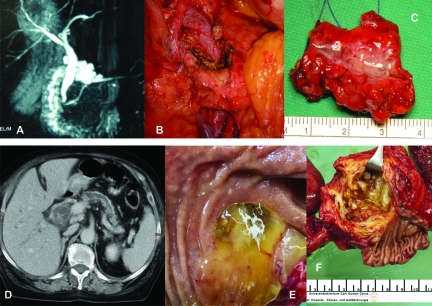
Pancreatic intraductal papillary mucinous neoplasms (IPMNs) rank among the most common cystic tumors of the pancreas. For a long time they were misdiagnosed as mucinous cystadenocarcinoma, ductal adenocarcinoma in situ, or chronic pancreatitis. Only in recent years have IPMNs been fully recognized as clinical and pathological entities, although their origin and molecular pathogenesis remain poorly understood. IPMNs are precursors of invasive carcinomas. When resected in a preinvasive state patient prognosis is excellent, and even when they are already invasive, patient prognosis is more favorable than with ductal adenocarcinomas. Subdivision into macroscopic and microscopic subtypes facilitates further patient risk stratification and directly impacts treatment. There are main duct and branch duct IPMNs, with the main duct type including the intestinal, pancreatobiliary, and oncocytic types and the branch duct type solely harboring the gastric type. Whereas main duct IPMNs have a high risk for malignant progression, demanding their resection, branch duct IPMNs have a much lower risk for harboring malignancy. Patients with small branch duct/gastric-type IPMNs (<2 cm) without symptoms or mural nodules can be managed by periodic surveillance.
Conflict of interest statement
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the authors or independent peer reviewers.
Figures
References
-
- Kosmahl M, Pauser U, Anlauf M, et al. [Cystic pancreas tumors and their classification: Features old and new] Pathologe. 2005;26:22–30. - PubMed
-
- Ohhashi K, Murakami Y, Maruyama M, et al. Four cases of mucous secreting pancreatic cancer. Prog Digest Endosc. 1982;20:348–351.
-
- Morohoshi T, Kanda M, Asanuma K, et al. Intraductal papillary neoplasms of the pancreas. A clinicopathologic study of six patients. Cancer. 1989;64:1329–1335. - PubMed
-
- Klöppel G, Solcia E, Longnecker DS, et al. Second Edition. New York: Springer-Verlag; 1998. Histological Typing of Tumours of the Exocrine Pancreas: World Health Organization International Histological Classification of Tumours.
-
- Kosmahl M, Pauser U, Peters K, et al. Cystic neoplasms of the pancreas and tumor-like lesions with cystic features: A review of 418 cases and a classification proposal. Virchows Arch. 2004;445:168–178. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
