

Derivation, validation, and evaluation of a new QRISK model to estimate lifetime risk of cardiovascular disease: cohort study using QResearch database
- PMID: 21148212
- PMCID: PMC2999889
- DOI: 10.1136/bmj.c6624
Derivation, validation, and evaluation of a new QRISK model to estimate lifetime risk of cardiovascular disease: cohort study using QResearch database
Abstract
Objective: To develop, validate, and evaluate a new QRISK model to estimate lifetime risk of cardiovascular disease.
Design: Prospective cohort study with routinely collected data from general practice. Cox proportional hazards models in the derivation cohort to derive risk equations accounting for competing risks. Measures of calibration and discrimination in the validation cohort.
Setting: 563 general practices in England and Wales contributing to the QResearch database.
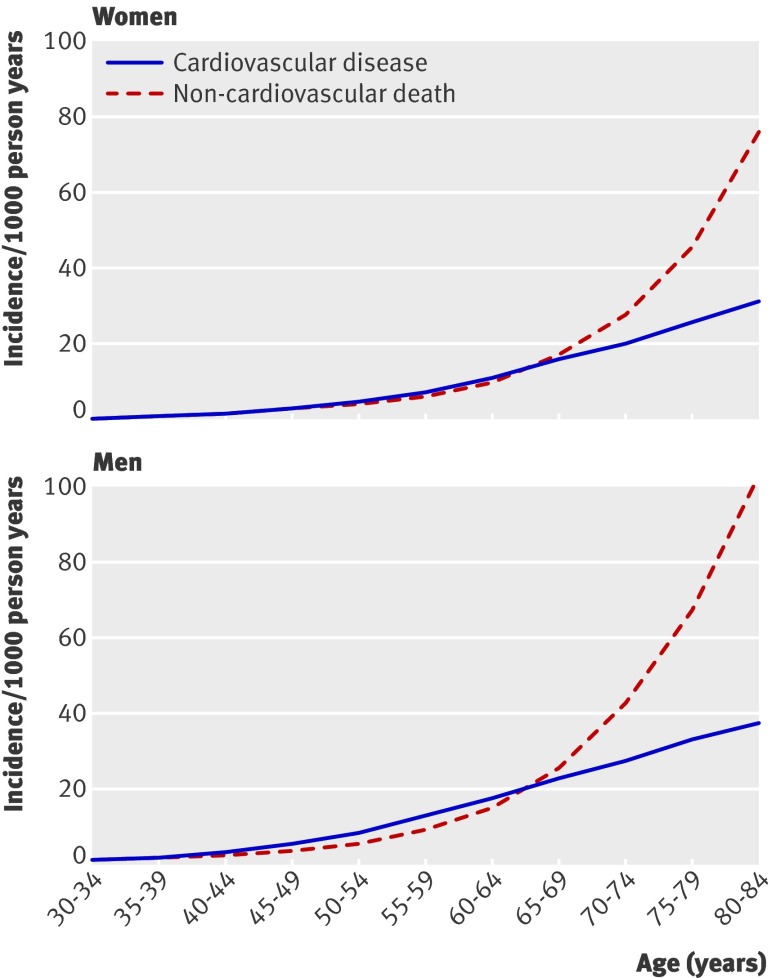
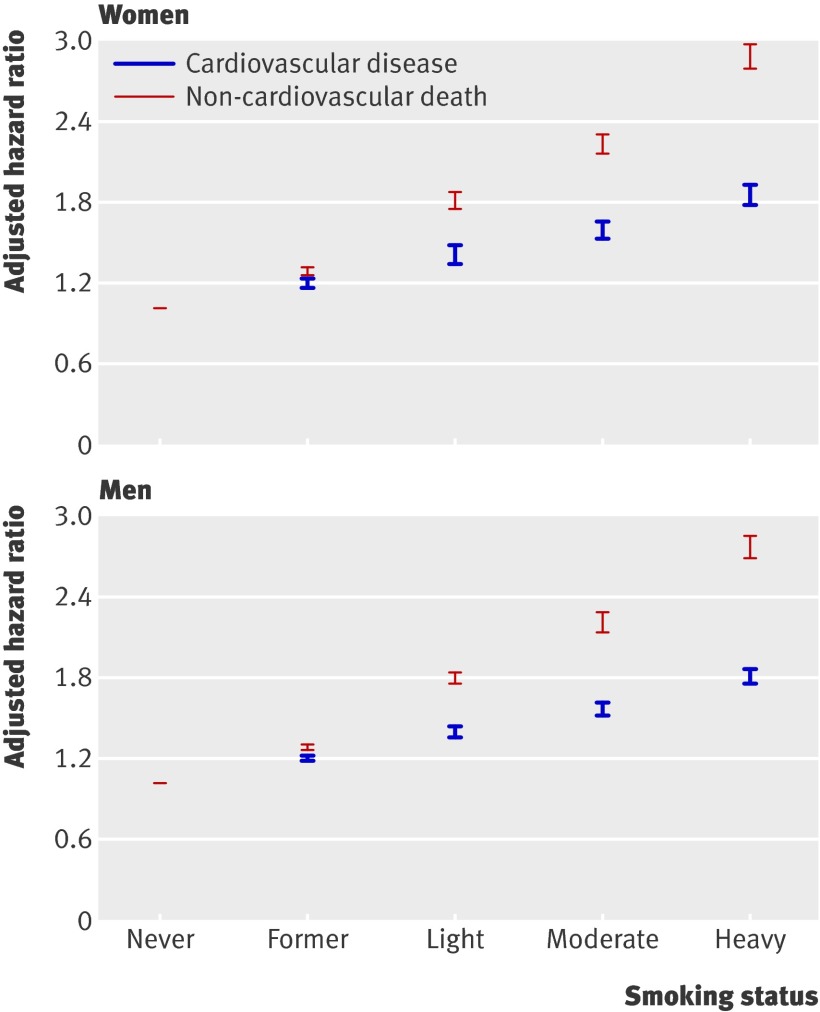
Subjects: Patients aged 30-84 years who were free of cardiovascular disease and not taking statins between 1 January 1994 and 30 April 2010: 2 343 759 in the derivation dataset, and 1 267 159 in the validation dataset. Main outcomes measures Individualised estimate of lifetime risk of cardiovascular disease accounting for smoking status, ethnic group, systolic blood pressure, ratio of total cholesterol:high density lipoprotein cholesterol, body mass index, family history of coronary heart disease in first degree relative aged <60 years, Townsend deprivation score, treated hypertension, rheumatoid arthritis, chronic renal disease, type 2 diabetes, and atrial fibrillation. Age-sex centile values for lifetime cardiovascular risk compared with 10 year risk estimated using QRISK2 (2010).
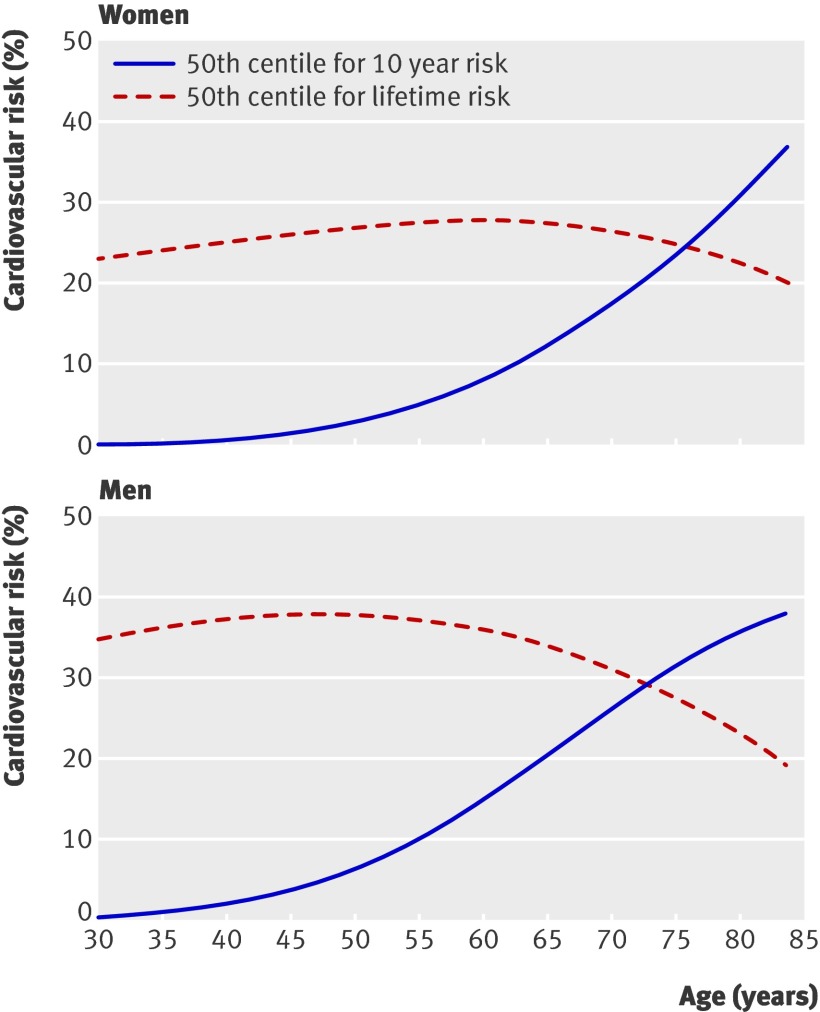
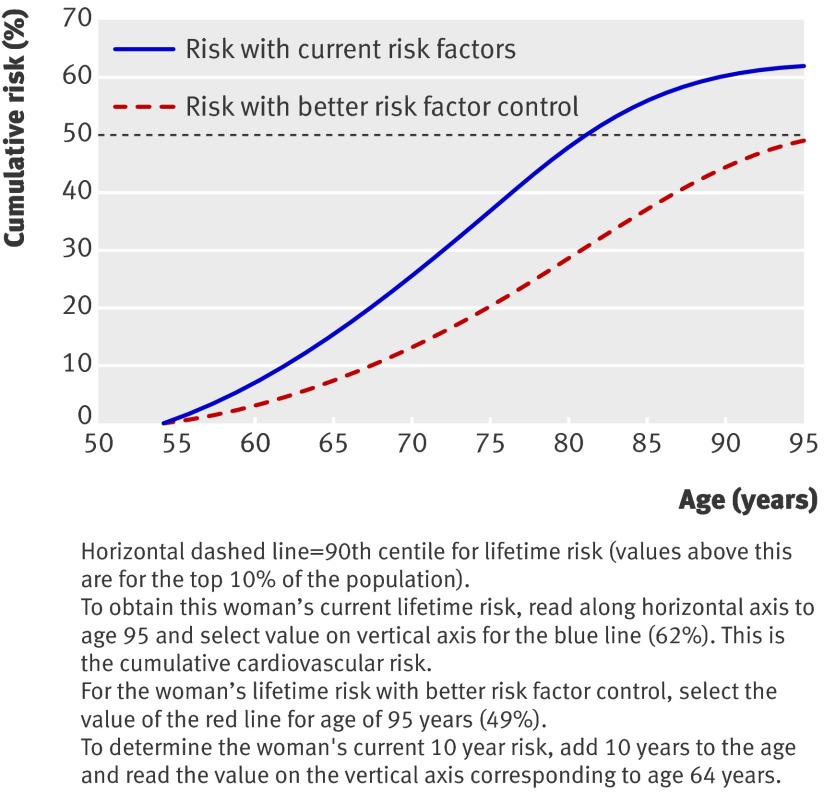
Results: Across all the 1 267 159 patients in the validation dataset, the 50th, 75th, 90th, and 95th centile values for lifetime risk were 31%, 39%, 50%, and 57% respectively. Of the 10% of patients in the validation cohort classified at highest risk with either the lifetime risk model or the 10 year risk model, only 18 385(14.5%) were at high risk on both measures. Patients identified as high risk with the lifetime risk approach were more likely to be younger, male, from ethnic minority groups, and have a positive family history of premature coronary heart disease than those identified with the 10 year QRISK2 score. The lifetime risk calculator is available at www.qrisk.org/lifetime/.
Conclusions: Compared with using a 10 year QRISK2 score, a lifetime risk score will tend to identify patients for intervention at a younger age. Although lifestyle interventions at an earlier age could be advantageous, there would be small gains under the age of 65, and medical interventions carry risks as soon as they are initiated. Research is needed to examine closely the cost effectiveness and acceptability of such an approach.
Conflict of interest statement
Competing interests: JH-C is professor of clinical epidemiology at the University of Nottingham and codirector of QResearch—a not-for-profit organisation that is a joint partnership between the University of Nottingham and EMIS (leading commercial supplier of information technology for 60% of general practices in the UK). JH-C is also director of ClinRisk, which produces open and closed source software to ensure the reliable and updatable implementation of clinical risk algorithms within clinical computer systems to help improve patient care. CC is associate professor of medical statistics at the University of Nottingham and a consultant statistician for ClinRisk. JR and PB have received no financial support for undertaking this work. JR and PB were previously members of the NICE Guideline Development Group for Lipid Modification, of which JR was chair. This work and any views expressed within it are solely those of the co-authors and not of any affiliated bodies or organisations. There are no other relationships or activities that could have influenced the submitted work.
Figures
Comment in
-
Is estimating lifetime cardiovascular risk useful?BMJ. 2010 Dec 31;341:c7379. doi: 10.1136/bmj.c7379. BMJ. 2010. PMID: 21196484 No abstract available.
-
Prevention: A new model to estimate lifetime risk of CVD.Nat Rev Cardiol. 2011 Feb;8(2):66. doi: 10.1038/nrcardio.2010.221. Nat Rev Cardiol. 2011. PMID: 21348147 No abstract available.
References
-
- British Heart Foundation. Coronary heart disease statistics. British Heart Foundation, 2007.
-
- Department of Health. Putting prevention first—vascular checks: risk assessment and management. DoH, 2008:15.
-
- NICE clinical guideline 64. Lipid modification—Cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. NICE, 2008. - PubMed
-
- Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3140-1. - PubMed
-
- Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R, et al. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Eur Heart J 2007;28:2375-414. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous